You might also like
- Disasters and Mass Casualty Incidents: The Nuts and Bolts of Preparedness and Response to Protracted and Sudden Onset EmergenciesFrom EverandDisasters and Mass Casualty Incidents: The Nuts and Bolts of Preparedness and Response to Protracted and Sudden Onset EmergenciesMauricio LynnNo ratings yet
- Rash BookDocument12 pagesRash BookPhoebe UsmleNo ratings yet
- Diagnostic Features of Disease: Based on French's Index of Differential DiagnosisFrom EverandDiagnostic Features of Disease: Based on French's Index of Differential DiagnosisRating: 1 out of 5 stars1/5 (1)
- Psychiatry Chapter 3Document54 pagesPsychiatry Chapter 3Online Money In EthiopiaNo ratings yet
- Pediatric Heart Transplantation: ISHLT Monograph Series, Volume 13From EverandPediatric Heart Transplantation: ISHLT Monograph Series, Volume 13No ratings yet
- Breast Milk Jaundice - JPG 2Document13 pagesBreast Milk Jaundice - JPG 2asmaaNo ratings yet
- Anesthesia for Congenital Heart DiseaseFrom EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerNo ratings yet
- Emergency Medicine Simulation Workbook: A Tool for Bringing the Curriculum to LifeFrom EverandEmergency Medicine Simulation Workbook: A Tool for Bringing the Curriculum to LifeTraci L. ThoureenNo ratings yet
- Public FRCEM Examination Report 2019Document23 pagesPublic FRCEM Examination Report 2019HossamNo ratings yet
- HEATS TRIAGE MANUAL TITLEDocument66 pagesHEATS TRIAGE MANUAL TITLEFitri SyawalNo ratings yet
- 2020 Acls Megacode Testing Scenarios - 2Document13 pages2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNo ratings yet
- Critical Care SedationFrom EverandCritical Care SedationAngelo Raffaele De GaudioNo ratings yet
- BLS Study Guide 020620013Document38 pagesBLS Study Guide 020620013R RatheeshNo ratings yet
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiNo ratings yet
- Emergency Ortho BCS 2017Document80 pagesEmergency Ortho BCS 2017Priza RazunipNo ratings yet
- HerniaDocument13 pagesHerniarmt_01No ratings yet
- Antrim ED Handbook 2019Document238 pagesAntrim ED Handbook 2019Chris Jardine LiNo ratings yet
- Pneumothorax Diagnosis & TreatmentDocument95 pagesPneumothorax Diagnosis & Treatmentnaveen vennilavanNo ratings yet
- ACLS Protocols Pocket VersionDocument2 pagesACLS Protocols Pocket Versionjohndoe1995No ratings yet
- CPT Case 4 PneumoniaDocument7 pagesCPT Case 4 PneumoniaAskine Jiezl Ico TadeoNo ratings yet
- Neonatal Jaundice NotesDocument5 pagesNeonatal Jaundice NotesEros CuestaNo ratings yet
- Emergency MasterDocument8 pagesEmergency MasterSara M.GheryanNo ratings yet
- NURSING GUIDELINE - Version 1.0Document35 pagesNURSING GUIDELINE - Version 1.0hidayatNo ratings yet
- Practical Gastroenterology and Hepatology Board Review ToolkitFrom EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNo ratings yet
- Cardiac/Cardiogenic Shock: Clinical Practice GuidelinesDocument3 pagesCardiac/Cardiogenic Shock: Clinical Practice GuidelinesAnonymous Yo0mStNo ratings yet
- Acute Resuscitation and Crisis Management: Acute Critical Events Simulation (ACES)From EverandAcute Resuscitation and Crisis Management: Acute Critical Events Simulation (ACES)David NeilipovitzNo ratings yet
- Pulmo ThromboembolismDocument34 pagesPulmo ThromboembolismAlexander Santiago ParelNo ratings yet
- ECG in Emergency MedicineDocument228 pagesECG in Emergency MedicineM.FADLINo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- ICP Waveform Analysis: Understanding Intracranial Physiology & MonitoringDocument55 pagesICP Waveform Analysis: Understanding Intracranial Physiology & MonitoringMaddox EdeyajNo ratings yet
- ISHLT Guidelines for the Management of Pediatric Heart FailureFrom EverandISHLT Guidelines for the Management of Pediatric Heart FailureNo ratings yet
- ECG Interpretation DR - Rawan AlshreemDocument25 pagesECG Interpretation DR - Rawan AlshreemMarymii Al-sahlawiiNo ratings yet
- European Resuscitation Council Guidelines 2021Document468 pagesEuropean Resuscitation Council Guidelines 2021Khalid G. AzouniNo ratings yet
- Wellen EcgDocument9 pagesWellen EcgElokNo ratings yet
- PRES MCQsDocument218 pagesPRES MCQsdoctorbilalsNo ratings yet
- NEURO2 3.05 Neurosurgical Management of Stroke and CNS Infection - Dr. Domingo PDFDocument3 pagesNEURO2 3.05 Neurosurgical Management of Stroke and CNS Infection - Dr. Domingo PDFPatricia Nicole AlcarazNo ratings yet
- Pancoast TumorDocument26 pagesPancoast TumorDhanis HastinNo ratings yet
- 01 - Decision Making in Emergency MedicineDocument4 pages01 - Decision Making in Emergency MedicineSlvdrPlgrnNo ratings yet
- Practice Guidelines For Juniors 01 June 2016Document3 pagesPractice Guidelines For Juniors 01 June 2016ElaineNo ratings yet
- Initial Assessment and Management: Presented by Fayez Abillama, MDDocument53 pagesInitial Assessment and Management: Presented by Fayez Abillama, MDDaniel GhosseinNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Emergency MedicineDocument6 pagesEmergency MedicineAnnisa Agna PuspatamiNo ratings yet
- ST4 Emergency Medicine Person SpecificationDocument7 pagesST4 Emergency Medicine Person SpecificationQusaiBadrNo ratings yet
- Eusem Epi Guidelines March 2020 PDFDocument92 pagesEusem Epi Guidelines March 2020 PDFАлекс КейNo ratings yet
- CME Examination DermatologyDocument25 pagesCME Examination DermatologylimeddyNo ratings yet
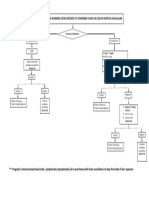
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- Approach To SyncopeDocument38 pagesApproach To SyncopeNurhafizah IbrahimNo ratings yet
- Indian Guidelines On Epilepsy: Mrinal Kanti Roy, Dhiman DasDocument6 pagesIndian Guidelines On Epilepsy: Mrinal Kanti Roy, Dhiman DasNurhafizah IbrahimNo ratings yet
- Cardinal Presentations Guide Hsas 21.11.2019Document20 pagesCardinal Presentations Guide Hsas 21.11.2019Nurhafizah IbrahimNo ratings yet
- Cardinal Presentations Guide Hsas 21.11.2019Document20 pagesCardinal Presentations Guide Hsas 21.11.2019Nurhafizah IbrahimNo ratings yet
- SuratDocument7 pagesSuratNurhafizah IbrahimNo ratings yet
- Dengue Fever Y.o/malay/ ULDocument9 pagesDengue Fever Y.o/malay/ ULNurhafizah IbrahimNo ratings yet
- PosttDocument1 pagePosttNurhafizah IbrahimNo ratings yet
- Cyber ParentingDocument1 pageCyber ParentingNurhafizah IbrahimNo ratings yet
- Apd M Sample ImportmDocument5 pagesApd M Sample ImportmNurhafizah IbrahimNo ratings yet
- Cyber ParentingDocument1 pageCyber ParentingNurhafizah IbrahimNo ratings yet
- Template Jadual WaktuDocument1 pageTemplate Jadual WaktuNurhafizah IbrahimNo ratings yet
- Latihan M6 Independent Sample T TestDocument1 pageLatihan M6 Independent Sample T TestNurhafizah IbrahimNo ratings yet
- Healthy Eating Habits GuidelineDocument30 pagesHealthy Eating Habits GuidelineSuhanidah MyNo ratings yet
- Cancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasDocument5 pagesCancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Csec Physics Sbaform ModerationDocument1 pageCsec Physics Sbaform Moderationapi-248240402No ratings yet
- Covid MemoDocument4 pagesCovid Memocharlie malalangNo ratings yet
- Outcomes Before and After Total Knee Arthroplasty Compared To Healthy AdultsDocument20 pagesOutcomes Before and After Total Knee Arthroplasty Compared To Healthy AdultsFirdaus Septhy ArdhyanNo ratings yet
- Worksheet For Respiration Low AnswersDocument2 pagesWorksheet For Respiration Low AnswersIcs 2022No ratings yet
- Wa0002.Document9 pagesWa0002.SojiNo ratings yet
- Bahan Kuliah MHM Beginning BioethicsDocument80 pagesBahan Kuliah MHM Beginning BioethicsKlarasita WibowoNo ratings yet
- Pianakafinal Sa Lahatt RyannDocument14 pagesPianakafinal Sa Lahatt RyannPaul IglesiasNo ratings yet
- Identification: Infosafe No.: LPSIZ Issued Date: 30/03/2015 Issued By: Sibelco Australia LimitedDocument7 pagesIdentification: Infosafe No.: LPSIZ Issued Date: 30/03/2015 Issued By: Sibelco Australia Limitedsentient.bean8226No ratings yet
- Benefits of Intermittent FastingDocument3 pagesBenefits of Intermittent FastingSaurabh PandeyNo ratings yet
- Module 1Document26 pagesModule 1priya malikNo ratings yet
- Respiratory and Circulatory Systems Activity SheetDocument7 pagesRespiratory and Circulatory Systems Activity SheetalexNo ratings yet
- Adult Male and Female Height To Weight Ratio Chart PDFDocument4 pagesAdult Male and Female Height To Weight Ratio Chart PDFAkd DeshmukhNo ratings yet
- OET 3 Reading Test 17 Part ADocument5 pagesOET 3 Reading Test 17 Part AAlice ChirilaNo ratings yet
- Triethanolamine Safety ReportDocument6 pagesTriethanolamine Safety ReportMaria Inês HarrisNo ratings yet
- Nicu DoccumentationDocument17 pagesNicu Doccumentationchaarvi100% (1)
- AFCAT Admit CardDocument7 pagesAFCAT Admit CardMuskan ShuklaNo ratings yet
- CWTS ProposalDocument5 pagesCWTS ProposalAllana de CastroNo ratings yet
- English 7 Q2 Module 1 1Document15 pagesEnglish 7 Q2 Module 1 1Jojam CarpioNo ratings yet
- HLTWHS002: Follow Safe Work Practices For Direct Client CareDocument75 pagesHLTWHS002: Follow Safe Work Practices For Direct Client CareThảo Nguyễn100% (2)
- Ashgate - Landscape Professional Practice PDFDocument281 pagesAshgate - Landscape Professional Practice PDFyondaimethunderNo ratings yet
- Mac Cosmetic CatalogDocument39 pagesMac Cosmetic CatalogCamy Herstig60% (5)
- Project Report On Health & Safety PDFDocument3 pagesProject Report On Health & Safety PDFAakash SolankiNo ratings yet
- ER Diagram ExerciseDocument2 pagesER Diagram ExerciseFarhana NaziraNo ratings yet
- D&D 5E - Homebrew - Class ProfligateDocument7 pagesD&D 5E - Homebrew - Class Profligate19931214No ratings yet
- MATERIAL SAFETY DATA SHEET 3M™ Novec ™ 1230 Fire Protection Fluid (FK-5-1-12)Document8 pagesMATERIAL SAFETY DATA SHEET 3M™ Novec ™ 1230 Fire Protection Fluid (FK-5-1-12)Juan LuisNo ratings yet
- Identification of Aerobic Pathogenic Bacteria Isolated From Ready-to-Eat Cakes Sold in Traditional Markets in Manado CityDocument3 pagesIdentification of Aerobic Pathogenic Bacteria Isolated From Ready-to-Eat Cakes Sold in Traditional Markets in Manado CityVenita NapitNo ratings yet
- 1.3 Cashew Nut. Doc Phuoc Long 24-SepDocument6 pages1.3 Cashew Nut. Doc Phuoc Long 24-SepPhuong NguyenNo ratings yet
- 의약품동등성시험기준 해설서 요약Document137 pages의약품동등성시험기준 해설서 요약Travis JeonNo ratings yet