You might also like
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- CT and MR Findings of Michel Anomaly: Inner Ear Aplasia: Case ReportDocument4 pagesCT and MR Findings of Michel Anomaly: Inner Ear Aplasia: Case ReportEBE THTNo ratings yet
- Congenital Agenesis of All The Nasal Cartilages: Casereport Craniofacial/MaxillofacialDocument3 pagesCongenital Agenesis of All The Nasal Cartilages: Casereport Craniofacial/MaxillofacialDiego A. Cuadros TorresNo ratings yet
- Imaging of Congenital Inner Ear Malformations: Poster No.: Congress: Type: AuthorsDocument21 pagesImaging of Congenital Inner Ear Malformations: Poster No.: Congress: Type: AuthorsKennedy NgoseyweNo ratings yet
- Congenital Malformations of Temporal Bone: by Dr. T. Balasubramanian M.S. D.L.ODocument16 pagesCongenital Malformations of Temporal Bone: by Dr. T. Balasubramanian M.S. D.L.OIvan DarioNo ratings yet
- MenereDocument11 pagesMenereJauhari JoNo ratings yet
- Incidental Reportzaharopoulos2000Document4 pagesIncidental Reportzaharopoulos2000maglangitmarvincNo ratings yet
- Imaging of Congenital Cholesteatoma With Atretic EarDocument4 pagesImaging of Congenital Cholesteatoma With Atretic EarVina AzrialNo ratings yet
- Embryology and Anatomy of The Earoperative Techniques in OtolaryngologyDocument23 pagesEmbryology and Anatomy of The Earoperative Techniques in OtolaryngologyAtrik PristicaNo ratings yet
- 2015 - Hildrew - A Newborn With Three Cochlear Turns Case Report and Literature ReviewDocument3 pages2015 - Hildrew - A Newborn With Three Cochlear Turns Case Report and Literature ReviewkingNo ratings yet
- Cleft Palate Patient With Conductive Hearing Loss Due To Stapes FixationDocument3 pagesCleft Palate Patient With Conductive Hearing Loss Due To Stapes Fixationintanmaryani9_943390No ratings yet
- Branchial Cleft Cyst: A Case Report and Review of LiteratureDocument3 pagesBranchial Cleft Cyst: A Case Report and Review of LiteratureValonia IreneNo ratings yet
- Human Malformations - 11 - NoseDocument17 pagesHuman Malformations - 11 - NoseAhmed H. Ali ElbestaweyNo ratings yet
- Management of Congenital Microtia With Meatoplasty and TympanoplastyDocument9 pagesManagement of Congenital Microtia With Meatoplasty and TympanoplastyismailyNo ratings yet
- Case Report: Matin Ghazizade, Mahboobe Asadi and Pouyan DarbaniDocument4 pagesCase Report: Matin Ghazizade, Mahboobe Asadi and Pouyan DarbanirizkiaNo ratings yet
- Human Malformations - 10 - EarDocument45 pagesHuman Malformations - 10 - EarAhmed H. Ali ElbestaweyNo ratings yet
- Aggressive Papillary Tumor of The Middle Ear: A True Entity or An Endolymphatic Sac Neoplasm?Document4 pagesAggressive Papillary Tumor of The Middle Ear: A True Entity or An Endolymphatic Sac Neoplasm?Umitha Rahmi SaniNo ratings yet
- Amniotic Band SyndromeDocument5 pagesAmniotic Band SyndromeganotNo ratings yet
- Bilateral Nasolabial Cyst MarcoviceanuDocument4 pagesBilateral Nasolabial Cyst MarcoviceanubamsusiloNo ratings yet
- Chapter 26Document8 pagesChapter 26Saurabh SatheNo ratings yet
- Trifonia Astri Fergaus B - Eposter Frontoethmoidal Meningoencephalocele (Fullpaper) - EDITDocument6 pagesTrifonia Astri Fergaus B - Eposter Frontoethmoidal Meningoencephalocele (Fullpaper) - EDITtrifoniastriNo ratings yet
- Embryology and Anatomy of The Ear: Lauren B. Moneta, MD, Lourdes Quintanilla-Dieck, MDDocument6 pagesEmbryology and Anatomy of The Ear: Lauren B. Moneta, MD, Lourdes Quintanilla-Dieck, MDsandranavarro27No ratings yet
- Imaging of PediatricHearing LossDocument13 pagesImaging of PediatricHearing LossDianithus169No ratings yet
- Nakajima 2015Document9 pagesNakajima 2015Carturo VduncanNo ratings yet
- Mca/Mr: New Syndrome?Document3 pagesMca/Mr: New Syndrome?JoNo ratings yet
- 23 Hearing - Outer Ear Development - EmbryologyDocument10 pages23 Hearing - Outer Ear Development - Embryologysolikin ikinNo ratings yet
- Median (Third) Occipital CondyleDocument4 pagesMedian (Third) Occipital Condylespin_echoNo ratings yet
- Larsens Human Embryology 468 495Document28 pagesLarsens Human Embryology 468 495Bintang PutraNo ratings yet
- Embryology of EarDocument32 pagesEmbryology of EarAnsuman SahuNo ratings yet
- Lee 2018Document4 pagesLee 2018Yogi Putra Adhi PradanaNo ratings yet
- Anatomyofthe Auditory SystemDocument6 pagesAnatomyofthe Auditory System32. Nguyễn Tiến Thái SơnNo ratings yet
- Orthodontic Space Closure in A Young Female Patient With Solitary Median Maxillary Central Incisor SyndromeDocument15 pagesOrthodontic Space Closure in A Young Female Patient With Solitary Median Maxillary Central Incisor SyndromeRicha AhlawatNo ratings yet
- Bilateral Glomus Tympanicum Tumors: Human Temporalbone StudyDocument2 pagesBilateral Glomus Tympanicum Tumors: Human Temporalbone StudyEdy MorarNo ratings yet
- Cholesteatoma of External Auditory CanalDocument5 pagesCholesteatoma of External Auditory CanallolNo ratings yet
- CHILDRENDocument8 pagesCHILDRENÉrick JuárezNo ratings yet
- Inner Ear Schwannoma - Publication by DR Tarek Khrais - Medics Index MemberDocument4 pagesInner Ear Schwannoma - Publication by DR Tarek Khrais - Medics Index MemberMedicsindex Telepin Slidecase100% (2)
- Supposed Otolaryngology Emergency Which Presents Late Bilateral Congenital Choanal AtresiaDocument3 pagesSupposed Otolaryngology Emergency Which Presents Late Bilateral Congenital Choanal AtresiaPaul HartingNo ratings yet
- Microtia and Congenital Aural AtresiaDocument20 pagesMicrotia and Congenital Aural Atresiaapi-19500641No ratings yet
- Enlarged Vestibular AqueductDocument86 pagesEnlarged Vestibular AqueductGhada WageihNo ratings yet
- Middle and Posterior Fossa AspergillomaDocument4 pagesMiddle and Posterior Fossa AspergillomamuhammadNo ratings yet
- Excision of Branchial Cleft CystsDocument10 pagesExcision of Branchial Cleft Cystssjs315No ratings yet
- THT OmskDocument4 pagesTHT OmskLianaNo ratings yet
- Three-Dimensional Assessment of The Temporal Bone and Mandible Deformations in Patients With Congenital Aural AtresiaDocument3 pagesThree-Dimensional Assessment of The Temporal Bone and Mandible Deformations in Patients With Congenital Aural AtresiaAdarsh GhoshNo ratings yet
- 1 s2.0 S1672293009500025 MainDocument8 pages1 s2.0 S1672293009500025 Main273046236No ratings yet
- Glomus TympanicumDocument4 pagesGlomus TympanicumdiegoNo ratings yet
- Oncology of ENTDocument4 pagesOncology of ENTAlgivar Dial Prima DaudNo ratings yet
- Cosmetic Otoplasty 2018 DBDocument11 pagesCosmetic Otoplasty 2018 DBcirugia plastica uisNo ratings yet
- CP TumorsDocument21 pagesCP TumorsDr. T. Balasubramanian100% (4)
- ENT MCQforstudents AnswersDocument30 pagesENT MCQforstudents AnswersOlaNo ratings yet
- A Study of Auricle Morphology For Identification in IndiansDocument8 pagesA Study of Auricle Morphology For Identification in IndiansRohin GargNo ratings yet
- 18Document21 pages18SophiaNo ratings yet
- Case Report: A Rare Stapes AbnormalityDocument4 pagesCase Report: A Rare Stapes AbnormalityCarolina UrrutiaNo ratings yet
- Khoury 2002Document5 pagesKhoury 2002shu DuNo ratings yet
- SAMS: Provisionally Unique Multiple CongenitalDocument5 pagesSAMS: Provisionally Unique Multiple Congenitaljahfdfgsdjad asdhsajhajdkNo ratings yet
- 1817 Full PDFDocument7 pages1817 Full PDFNina Fera UtariNo ratings yet
- Congenital Isolated Aplasia of Lower Lateral Cartilage and Reconstruction Using Dorsal Hump MaterialDocument3 pagesCongenital Isolated Aplasia of Lower Lateral Cartilage and Reconstruction Using Dorsal Hump MaterialDiego A. Cuadros TorresNo ratings yet
- Meningioma of The Internal Auditory Canal Case ReportDocument4 pagesMeningioma of The Internal Auditory Canal Case ReportStanley KambeyNo ratings yet
- Conductive Hearing Loss With An Intact Tympanic Membrane: Diagnosed ApproachesDocument5 pagesConductive Hearing Loss With An Intact Tympanic Membrane: Diagnosed ApproachesMonika ZikraNo ratings yet
- The Developing Anterior Skull Base: CT Appearance From Birth To 2 Years of AgeDocument8 pagesThe Developing Anterior Skull Base: CT Appearance From Birth To 2 Years of AgeKumaran Bagavathi RagavanNo ratings yet
- External CholesteatomDocument5 pagesExternal CholesteatomIvana SupitNo ratings yet
- DF 12 Cochlear Apalsia and Cochlear HypoplasiaDocument3 pagesDF 12 Cochlear Apalsia and Cochlear HypoplasiaHendra SalehNo ratings yet
- Neurosurgery 3 1059Document4 pagesNeurosurgery 3 1059mirabelladonnaNo ratings yet
- DF 9 Review of Congenital Inner Ear Abnormalities On CT TemporalDocument5 pagesDF 9 Review of Congenital Inner Ear Abnormalities On CT TemporalHendra SalehNo ratings yet
- Tuberculous Spondylitis After Vertebral Augmentation: A Case Report With A Literature ReviewDocument9 pagesTuberculous Spondylitis After Vertebral Augmentation: A Case Report With A Literature ReviewHendra SalehNo ratings yet
- Kupon Bazar Amsa SparclingDocument2 pagesKupon Bazar Amsa SparclingHendra SalehNo ratings yet
- 2 - Kidney TraumaDocument72 pages2 - Kidney TraumaHendra SalehNo ratings yet
- Jadwal Rotasi Dan Jaga Coass Bedah 31-6 April 2019Document4 pagesJadwal Rotasi Dan Jaga Coass Bedah 31-6 April 2019fendiNo ratings yet
- Jadwal Jaga THT 2Document5 pagesJadwal Jaga THT 2Hendra SalehNo ratings yet
- Jadwal Jaga THTDocument5 pagesJadwal Jaga THTHendra SalehNo ratings yet
- Diagnosis Fisik Abdomen UNTADDocument20 pagesDiagnosis Fisik Abdomen UNTADHendra SalehNo ratings yet
- Amsa RingkasDocument12 pagesAmsa RingkasHendra SalehNo ratings yet
- Amsa RingkasDocument12 pagesAmsa RingkasHendra SalehNo ratings yet
- 677 Hi - Fi System ProfessionalDocument2 pages677 Hi - Fi System ProfessionalMarko MarkoNo ratings yet
- Audiometer Impedqnce Audiometer AT235 - USER - MANUALDocument103 pagesAudiometer Impedqnce Audiometer AT235 - USER - MANUALKafina Multi SejahteraNo ratings yet
- CP 99-2003 PreviewDocument9 pagesCP 99-2003 PreviewAquiles_voyNo ratings yet
- Vibrant Soundbridge ® Implantable Hearing System: Kristin M. Avitabile, MS, CCC-ADocument35 pagesVibrant Soundbridge ® Implantable Hearing System: Kristin M. Avitabile, MS, CCC-AsemiragaNo ratings yet
- Deaf CultureDocument17 pagesDeaf Cultureapi-385151452No ratings yet
- Late Diagnosis of Congenital Hearing Impairment in Children - The Parents' Experiences and OpinionsDocument10 pagesLate Diagnosis of Congenital Hearing Impairment in Children - The Parents' Experiences and OpinionsDwi KhoirriyaniNo ratings yet
- Class 9 Science Sound NCERT Notes PDFDocument8 pagesClass 9 Science Sound NCERT Notes PDFSulveNo ratings yet
- Sound Affects BookDocument44 pagesSound Affects Booknora100% (1)
- Chapter 26 NotesDocument106 pagesChapter 26 NotesFrancesca D'AnnunzioNo ratings yet
- Informazione Multimediale - Audio - : Lecture 1: Sound & Digital AudioDocument52 pagesInformazione Multimediale - Audio - : Lecture 1: Sound & Digital AudioMichele FioriNo ratings yet
- Sudden DeafnessDocument4 pagesSudden DeafnessferaNo ratings yet
- Histograma de Ruído - SimpsonDocument12 pagesHistograma de Ruído - SimpsonGustavo VieiraNo ratings yet
- Lesson Plan: Gyan Bharati School Saket, New DelhiDocument6 pagesLesson Plan: Gyan Bharati School Saket, New DelhiDivanshi ShakyaNo ratings yet
- Laboratory Experiment No. 2Document6 pagesLaboratory Experiment No. 2Aubrey RamiloNo ratings yet
- Sound Analysis and Noise Control - John Foreman PDFDocument472 pagesSound Analysis and Noise Control - John Foreman PDFJose Luis Arredondo RNo ratings yet
- Pure ToneDocument58 pagesPure TonefadzzzNo ratings yet
- Astm E1704Document6 pagesAstm E1704SURULIAPPAN PREMKMARNo ratings yet
- Sound: B. Short/Long Answer Questions AnswerDocument6 pagesSound: B. Short/Long Answer Questions AnswerSayantan ChakrabortyNo ratings yet
- Audiogram: R: O Red L: X BlueDocument2 pagesAudiogram: R: O Red L: X BlueRisma ReskanangaNo ratings yet
- NIHLDocument13 pagesNIHLStanislaus Stanley SuhermanNo ratings yet
- Huntair Coplanar Silencer 1107Document2 pagesHuntair Coplanar Silencer 1107Tu Burin DtNo ratings yet
- Lesson 6: Sensorysystem Lesson 6.1: Sense of SightDocument6 pagesLesson 6: Sensorysystem Lesson 6.1: Sense of SightGlessy AlvaroNo ratings yet
- Siva SutraDocument197 pagesSiva Sutraaade100% (6)
- CBSE Class 8 Science WorksheetDocument3 pagesCBSE Class 8 Science WorksheetKULDEEP PALANo ratings yet
- Acess SNDocument4 pagesAcess SNFitriyani LvNo ratings yet
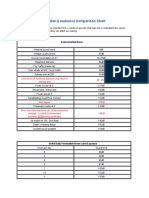
- Decibel (Loudness) Comparison Chart: Environmental NoiseDocument7 pagesDecibel (Loudness) Comparison Chart: Environmental NoiseMohsin Khan100% (1)
- Xbox Adaptive Controller en PT FR Es de Iw It PLDocument36 pagesXbox Adaptive Controller en PT FR Es de Iw It PLPãoComManteigaNo ratings yet
- Modern Mastering CMDocument19 pagesModern Mastering CMvickynampi100% (7)
- AKG d112 MkII CutsheetDocument2 pagesAKG d112 MkII CutsheetSebastian CasasNo ratings yet
- The Nature and Characteristics of SoundDocument52 pagesThe Nature and Characteristics of SoundJenimel TranquilleroNo ratings yet