You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Test Taking StratDocument43 pagesTest Taking StratRamon Carlo AlmiranezNo ratings yet
- Comparison of Icd 10 and DSM 5: BY Anitha J I Mphil Clinical PsychologyDocument102 pagesComparison of Icd 10 and DSM 5: BY Anitha J I Mphil Clinical Psychologyanitha1118No ratings yet
- Herbal Plants (Halamang Gamot)Document25 pagesHerbal Plants (Halamang Gamot)SORENI SORENINo ratings yet
- Icu Head To Toe AssessmentDocument3 pagesIcu Head To Toe Assessmentmsbunnilee100% (2)
- Ebook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFDocument67 pagesEbook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFroberto.duncan209100% (31)
- DRUG STUDY-1st BatchDocument27 pagesDRUG STUDY-1st BatchCanny CańasNo ratings yet
- Gram-Negative Bacteria TableDocument4 pagesGram-Negative Bacteria TablewingNo ratings yet
- Wilderness and Remote First Aid Pocket Guide PDFDocument2 pagesWilderness and Remote First Aid Pocket Guide PDFScott Kramer0% (2)
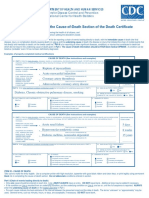
- Instructions For Completing The Cause of Death Section On Death Certificate PDFDocument2 pagesInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoNo ratings yet
- Club FootDocument46 pagesClub FootCarol Bruce100% (1)
- Retention Times For Records, Reports, and SpecimensDocument1 pageRetention Times For Records, Reports, and SpecimensDayledaniel SorvetoNo ratings yet
- PTSDDocument9 pagesPTSDAnisa Putri100% (1)
- Qué Es El Horror AutotxicusDocument5 pagesQué Es El Horror AutotxicusLuis Mundaca ZúñigaNo ratings yet
- Tier 1 CVSDocument23 pagesTier 1 CVSCHETHAN K SNo ratings yet
- HES007 Lab Session #15 SASDocument12 pagesHES007 Lab Session #15 SASJemimah GraceNo ratings yet
- 01 Introduction To DispensingDocument30 pages01 Introduction To DispensingRoselyn DawongNo ratings yet
- Colon CancerDocument25 pagesColon Cancerchori2008No ratings yet
- Pil 880 PDFDocument6 pagesPil 880 PDFBobbyNo ratings yet
- Holistic Goat Care: Table of ContentsDocument3 pagesHolistic Goat Care: Table of ContentsChelsea Green PublishingNo ratings yet
- Generic Name: Co-Amoxiclav Brand Name: Augmentin Classification: Dosage: 625 MGDocument6 pagesGeneric Name: Co-Amoxiclav Brand Name: Augmentin Classification: Dosage: 625 MGRoxanne Ganayo ClaverNo ratings yet
- Webinar 3 Exercise in PAD SlidesDocument46 pagesWebinar 3 Exercise in PAD SlidesRekha SatheesanNo ratings yet
- Adelola Adeloye Quintessential Neurological SurgeonDocument7 pagesAdelola Adeloye Quintessential Neurological SurgeonAnonymous 9QxPDpNo ratings yet
- Close Loop Medication ManagementDocument25 pagesClose Loop Medication Managementfathul jannahNo ratings yet
- Central Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsDocument33 pagesCentral Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsJoseph JohnNo ratings yet
- Concept Map RSVDocument1 pageConcept Map RSVNoemi GabayNo ratings yet
- Surgical Opening of Gutteral PouchhDocument32 pagesSurgical Opening of Gutteral PouchhAli KhanNo ratings yet
- Cold Pressure Test PDFDocument4 pagesCold Pressure Test PDFAdel LiaNo ratings yet
- 1 PDFDocument14 pages1 PDFBlackPork54No ratings yet
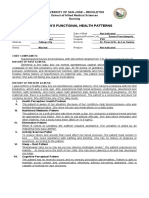
- Gordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingDocument2 pagesGordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- Walthauser H. Viaje, M.D., FpcsDocument1 pageWalthauser H. Viaje, M.D., FpcsRegine EnvidiadoNo ratings yet