You might also like
- COVID-19: Effects in Comorbidities and Special PopulationsFrom EverandCOVID-19: Effects in Comorbidities and Special PopulationsNo ratings yet
- Position Paper From The Indonesian Society of Thrombosis and Hemostasis (Inasth), Semarang Chapter: Management of Coagulopathy in Covid-19Document7 pagesPosition Paper From The Indonesian Society of Thrombosis and Hemostasis (Inasth), Semarang Chapter: Management of Coagulopathy in Covid-19eddy pasangkaNo ratings yet
- Pathogens 10 00370Document11 pagesPathogens 10 00370NS991No ratings yet
- Funciones y Actividades Plaquetarias Como Posibles Parámetros Hematológicos Relacionados Con La Enfermedad Por CoronavirusDocument7 pagesFunciones y Actividades Plaquetarias Como Posibles Parámetros Hematológicos Relacionados Con La Enfermedad Por CoronavirusEdinson Cortez VasquezNo ratings yet
- Position Paper From The InaSTHDocument7 pagesPosition Paper From The InaSTHwahyu suparnoNo ratings yet
- Blood 2020006000 PDFDocument21 pagesBlood 2020006000 PDFothilia.obadaNo ratings yet
- Thromboembolic Disease in COVID-19 Patients: A Brief Narrative ReviewDocument10 pagesThromboembolic Disease in COVID-19 Patients: A Brief Narrative ReviewSteven PutraNo ratings yet
- 2021 Article 546Document11 pages2021 Article 546Petru CarajaNo ratings yet
- Coagulop CovidDocument11 pagesCoagulop CovidbacchiocchipaoloNo ratings yet
- 2021 Page Covid-19 Thrombose Mecanismes TRDocument8 pages2021 Page Covid-19 Thrombose Mecanismes TRأمين الله القاضيNo ratings yet
- Viral CoagulopathyDocument7 pagesViral CoagulopathyGheavita Chandra DewiNo ratings yet
- Koc 2022Document14 pagesKoc 2022John GoranitisNo ratings yet
- Anticoagulant Treatment in COVID 19: A Narrative ReviewDocument7 pagesAnticoagulant Treatment in COVID 19: A Narrative ReviewossinNo ratings yet
- The Coagulopathy, Endotheliopathy, and Vasculitis of COVID 19Document9 pagesThe Coagulopathy, Endotheliopathy, and Vasculitis of COVID 19arif 2006No ratings yet
- COVID 19AndHematology IndiaDocument6 pagesCOVID 19AndHematology IndiaVandana SharmaNo ratings yet
- Gopalaswamy y Subbian - 2021 - Corticosteroids For COVID-19 Therapy Potential ImDocument18 pagesGopalaswamy y Subbian - 2021 - Corticosteroids For COVID-19 Therapy Potential ImOsmar SulcaNo ratings yet
- Cellbio - 2020060411193112 Covid - 19Document13 pagesCellbio - 2020060411193112 Covid - 19ahmed hussien kamelNo ratings yet
- Endothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionsDocument24 pagesEndothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionssamuelNo ratings yet
- Preprints202006 0062 v1Document13 pagesPreprints202006 0062 v1Hagar AlaaNo ratings yet
- D-Dimer As An Indicator of Prognosis in Sars-Cov-2 Infection: A Systematic ReviewDocument10 pagesD-Dimer As An Indicator of Prognosis in Sars-Cov-2 Infection: A Systematic ReviewIraNo ratings yet
- COVID-19 and Coagulopathy: Malay Sarkar - Irappa V. Madabhavi - Pham Nguyen Quy - Manjunath B. GovindagoudarDocument16 pagesCOVID-19 and Coagulopathy: Malay Sarkar - Irappa V. Madabhavi - Pham Nguyen Quy - Manjunath B. GovindagoudarsamuelNo ratings yet
- Mucormycosis PDFDocument4 pagesMucormycosis PDFiram shafiNo ratings yet
- Coagulopathy of Coronavirus Disease 2019: Review ArticlesDocument7 pagesCoagulopathy of Coronavirus Disease 2019: Review ArticlesBianca IlieNo ratings yet
- MAnaagement Koagulapati Dan Thrombolis Pada Pasien CovDocument13 pagesMAnaagement Koagulapati Dan Thrombolis Pada Pasien CovJuwita Rashi LumbantoruanNo ratings yet
- Jim 2020 0023 1Document5 pagesJim 2020 0023 1diaconuNo ratings yet
- 1 s2.0 S1156523321000585 MainDocument4 pages1 s2.0 S1156523321000585 MainAna PerfeitoNo ratings yet
- Pharmacotherapy in Covid 19 Potential Impact of Targeting The Complement SystemDocument12 pagesPharmacotherapy in Covid 19 Potential Impact of Targeting The Complement SystemDENiS ROSARIO CASABONA ACEVEDONo ratings yet
- SARS-CoV-2 and Coagulation Disorders in Different OrgansDocument11 pagesSARS-CoV-2 and Coagulation Disorders in Different OrgansMaarteeh' Listing Laambeert'No ratings yet
- Covid Induced CVDocument23 pagesCovid Induced CVriskiNo ratings yet
- D'Dimer, Fibrinogen Dan IL6 PAD CovidDocument8 pagesD'Dimer, Fibrinogen Dan IL6 PAD CovidWartimah imahNo ratings yet
- (IJCST-V10I5P29) :mrs R. Jhansi Rani, B. Karunakar ReddyDocument7 pages(IJCST-V10I5P29) :mrs R. Jhansi Rani, B. Karunakar ReddyEighthSenseGroupNo ratings yet
- 8 DBFDocument4 pages8 DBFFatimaNo ratings yet
- Anesthesia and COVID-19: What We Should Know and What We Should DoDocument11 pagesAnesthesia and COVID-19: What We Should Know and What We Should DoAfniNo ratings yet
- Assessment of Changes and Complications Caused by Coronavirus Infection in The Lungs Using Computed TomographyDocument6 pagesAssessment of Changes and Complications Caused by Coronavirus Infection in The Lungs Using Computed TomographyCentral Asian StudiesNo ratings yet
- Covid 19 Diagnostio e TerapiaDocument15 pagesCovid 19 Diagnostio e TerapiaJess ElizeuNo ratings yet
- Incidence of Deep Venous Thrombosis in Hospitalized COVID-19 Patients in Isolated de Martini Hospital Mogadishu SomaliaDocument8 pagesIncidence of Deep Venous Thrombosis in Hospitalized COVID-19 Patients in Isolated de Martini Hospital Mogadishu SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact Covid 19 UrologyDocument12 pagesImpact Covid 19 UrologyGasy ManjabeNo ratings yet
- Jama Wiersinga 2020 RV 200009 1597950376.62291Document12 pagesJama Wiersinga 2020 RV 200009 1597950376.62291Iziza LunaskhiNo ratings yet
- Stem Cell Based Therapy Option in COVID-19 - Is It Really Promising?Document17 pagesStem Cell Based Therapy Option in COVID-19 - Is It Really Promising?diana.alyNo ratings yet
- Sri Ratu Septini Farmasi 4B PDFDocument8 pagesSri Ratu Septini Farmasi 4B PDFWinanda SitinjakNo ratings yet
- COVID-19-Related Cardiovascular Disease and Practical Considerations For Perioperative CliniciansDocument11 pagesCOVID-19-Related Cardiovascular Disease and Practical Considerations For Perioperative CliniciansAprilia boddhiNo ratings yet
- 1479 6813 Jme 22 0036Document26 pages1479 6813 Jme 22 0036Hitesh VermaNo ratings yet
- COVID 19 and The StrokeDocument7 pagesCOVID 19 and The StrokeLone GhostNo ratings yet
- COVID 19, An Emerging Coronavirus Infection CurrentDocument8 pagesCOVID 19, An Emerging Coronavirus Infection CurrentAsepNo ratings yet
- An Evidence Based Case Study To Identify The Role of Bothrops Lanceolatus As A Homeopathic AnticoagulantDocument6 pagesAn Evidence Based Case Study To Identify The Role of Bothrops Lanceolatus As A Homeopathic AnticoagulantEditor IJTSRDNo ratings yet
- Cytokine Storm in COVID-19Document11 pagesCytokine Storm in COVID-19Feli FelNo ratings yet
- Clinical Infection in Practice: Aafiya Ambereen, Sajjad A. Rahman, Suhailur Rehman, Kamran Zaidi, S.H. ArifDocument6 pagesClinical Infection in Practice: Aafiya Ambereen, Sajjad A. Rahman, Suhailur Rehman, Kamran Zaidi, S.H. Ariffrans lazioNo ratings yet
- Tormenta de Citocinas SARS COVIDDocument5 pagesTormenta de Citocinas SARS COVIDjenith andradeNo ratings yet
- Endothelial Dysfunction and ImmunothrombosisDocument11 pagesEndothelial Dysfunction and ImmunothrombosisJob GonzagaNo ratings yet
- COVID 19 Associated Opportunistic Infections: A Snapshot On The Current ReportsDocument20 pagesCOVID 19 Associated Opportunistic Infections: A Snapshot On The Current ReportsAndreea CiorneaNo ratings yet
- Articulo 2. Cytokine Storm Intervention in The Early Stages of COVID-19 PneumoniaDocument5 pagesArticulo 2. Cytokine Storm Intervention in The Early Stages of COVID-19 PneumoniaYajaira MenesesNo ratings yet
- Cardiac Patients and COVID-19: What The General Practitioner Should KnowDocument4 pagesCardiac Patients and COVID-19: What The General Practitioner Should KnowDimas WahyudinataNo ratings yet
- Journal of Internal Medicine - 2020 - Pascarella - COVID 19 Diagnosis and Management A Comprehensive ReviewDocument15 pagesJournal of Internal Medicine - 2020 - Pascarella - COVID 19 Diagnosis and Management A Comprehensive ReviewOscar Oswaldo SCNo ratings yet
- Jaha 120 019650Document24 pagesJaha 120 019650nuvitaNo ratings yet
- PIIS2468024923012342Document26 pagesPIIS2468024923012342Jhair Murillo AparicioNo ratings yet
- Comprehensive Treatment COVID 19Document49 pagesComprehensive Treatment COVID 19ekoNo ratings yet
- Rheumatology: Implications of COVID 19 in Pediatric RheumatologyDocument21 pagesRheumatology: Implications of COVID 19 in Pediatric RheumatologyLaira VillalobosNo ratings yet
- Journal Pre-Proof: Life SciencesDocument20 pagesJournal Pre-Proof: Life Sciences3323No ratings yet
- Lymphocytopenia and COVID19 A Literature ReviewDocument5 pagesLymphocytopenia and COVID19 A Literature ReviewEditor IJTSRDNo ratings yet
- Use Only: Pulmonary Involvement and Cytochemical Storm: Beyond Sars-Cov-2 PneumoniaeDocument3 pagesUse Only: Pulmonary Involvement and Cytochemical Storm: Beyond Sars-Cov-2 PneumoniaeIsaac VergaraNo ratings yet
- S Shapiro VTE Prevention AND COVID ThrombosisUK May 2020Document22 pagesS Shapiro VTE Prevention AND COVID ThrombosisUK May 2020Ririn Efsa JutiaNo ratings yet
- Misdiagnosis in Covid19 Era JACC PDFDocument6 pagesMisdiagnosis in Covid19 Era JACC PDFRirin Efsa JutiaNo ratings yet
- Covid19 Treatmentguidelines NIHDocument146 pagesCovid19 Treatmentguidelines NIHRirin Efsa JutiaNo ratings yet
- Barnes2020 Article ThromboembolismAndAnticoagulanDocument10 pagesBarnes2020 Article ThromboembolismAndAnticoagulanRirin Efsa JutiaNo ratings yet
- ACC153 Cheat Sheet 7Document7 pagesACC153 Cheat Sheet 7TIRTAYUDA MUNGGARANANo ratings yet
- Jurding DR SaugiDocument44 pagesJurding DR SaugiDian FitriNo ratings yet
- Seltzer and Benders Dental Pulp 2012 - 1-118-120Document3 pagesSeltzer and Benders Dental Pulp 2012 - 1-118-120Karina HernandezNo ratings yet
- 166 23asl02-8388Document6 pages166 23asl02-8388CARLIN JOSH MENDOZANo ratings yet
- Pathology Book - Chapter 2 - Inflammation - HKDocument12 pagesPathology Book - Chapter 2 - Inflammation - HKagar agarNo ratings yet
- Neutrophil Function - From Mechanisms To DiseaseDocument33 pagesNeutrophil Function - From Mechanisms To DiseaseCristianNo ratings yet
- 7structural Organization in Animals PDFDocument8 pages7structural Organization in Animals PDFDharmendra SinghNo ratings yet
- ANGIOSARCOMA A Rare Cause of Pleural MalignancyDocument3 pagesANGIOSARCOMA A Rare Cause of Pleural MalignancyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- FocDocument336 pagesFocRuban DanielNo ratings yet
- Acute InflammationDocument47 pagesAcute InflammationAjit Metake-DeshmukhNo ratings yet
- Inflammation and RepairDocument34 pagesInflammation and Repairanshum guptaNo ratings yet
- Prof Qaisar Khan TrialsDocument56 pagesProf Qaisar Khan TrialsAsim NajamNo ratings yet
- Superhuman at 70!Document28 pagesSuperhuman at 70!Fortune IkelianiNo ratings yet
- Extracellular Vimentin Mimics VEGF and Is A Target For Anti-Angiogenic ImmunotherapyDocument20 pagesExtracellular Vimentin Mimics VEGF and Is A Target For Anti-Angiogenic ImmunotherapyElse HuijbersNo ratings yet
- 9a Pathology PDFDocument47 pages9a Pathology PDFDianne GalangNo ratings yet
- Lecture On Hemodynamic and Thromboembolic DisordersDocument77 pagesLecture On Hemodynamic and Thromboembolic DisordersCharmaine Torio PastorNo ratings yet
- Forever Living ARGIv 2Document4 pagesForever Living ARGIv 2Mainul Islam SharifNo ratings yet
- Drug-Induced Lung Toxicity: Journal MaryDocument17 pagesDrug-Induced Lung Toxicity: Journal MaryMadihah shawalNo ratings yet
- NIMCET MCA Entrance 2011 Solved Question PaperDocument12 pagesNIMCET MCA Entrance 2011 Solved Question PaperArnabNo ratings yet
- Invited Review: Mechanisms of Normal and Tumor-Derived AngiogenesisDocument24 pagesInvited Review: Mechanisms of Normal and Tumor-Derived AngiogenesisDrMohit SharmaNo ratings yet
- Flores Et Al 2002 L-ArgininaDocument9 pagesFlores Et Al 2002 L-ArgininaJorge ParodiNo ratings yet
- Obesity Related Cognitive Impairment The Role of Endo - 2019 - Neurobiology ofDocument18 pagesObesity Related Cognitive Impairment The Role of Endo - 2019 - Neurobiology ofSabrina YenNo ratings yet
- Mechanism of Tissue RepairDocument22 pagesMechanism of Tissue RepairWalidad AarbiNo ratings yet
- Vet PathologyDocument128 pagesVet PathologyMegarsaNo ratings yet
- Menopause - A Cardiometabolic Transition (Nappi Et Al., 2022)Document14 pagesMenopause - A Cardiometabolic Transition (Nappi Et Al., 2022)Susana RoyNo ratings yet
- 12 Blood VesselsDocument26 pages12 Blood VesselsBalaji DNo ratings yet
- Hyperbaric Soft Tissue RadionecrosisDocument13 pagesHyperbaric Soft Tissue Radionecrosisina permata dewiNo ratings yet
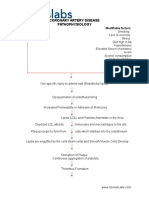
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps50% (4)
- Neutrophil Biology: C Carmona-Rivera and MJ Kaplan, National Institutes of Health, Bethesda, MD, USADocument9 pagesNeutrophil Biology: C Carmona-Rivera and MJ Kaplan, National Institutes of Health, Bethesda, MD, USAbNo ratings yet
- Magnetic Iron Oxide Nanoparticles For Imaging, Targeting and Treatment of Primary and Metastatic Tumors of The BrainDocument19 pagesMagnetic Iron Oxide Nanoparticles For Imaging, Targeting and Treatment of Primary and Metastatic Tumors of The BrainGurvinder SinghNo ratings yet