You might also like
- New Antibiotics For Community-Acquired Pneumonia: ReviewDocument7 pagesNew Antibiotics For Community-Acquired Pneumonia: ReviewAndhika HamdanyNo ratings yet
- Intravenous Immunoglobulin For Adjunctive.2Document6 pagesIntravenous Immunoglobulin For Adjunctive.2Anne RobinsonNo ratings yet
- Treatment of Fever in Neutropenia in Pediatric Oncology PatientsDocument6 pagesTreatment of Fever in Neutropenia in Pediatric Oncology PatientsRaíla SoaresNo ratings yet
- Antifungal Use in The Surgical ICU Patient: ReviewDocument8 pagesAntifungal Use in The Surgical ICU Patient: ReviewenriquegarciagalianaNo ratings yet
- Economic Evaluation Alongside The Probiotics To Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT) : Study ProtocolDocument8 pagesEconomic Evaluation Alongside The Probiotics To Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT) : Study ProtocolSharan SahotaNo ratings yet
- JIR 306849 N Acetylcysteine As Adjuvant Therapy For Covid 19 Ndash ADocument21 pagesJIR 306849 N Acetylcysteine As Adjuvant Therapy For Covid 19 Ndash ARefa OktoyardaNo ratings yet
- Acscentsci 1c00120Document22 pagesAcscentsci 1c00120Beverly EstoqueNo ratings yet
- Cochrane ChloroquineDocument18 pagesCochrane ChloroquineTomasz KoboszNo ratings yet
- Secondary Pneumonias in Critically Ill Patients.4Document6 pagesSecondary Pneumonias in Critically Ill Patients.4FIA SlotNo ratings yet
- Guidelines For Severe CapDocument6 pagesGuidelines For Severe CapReynaldoBinsarNo ratings yet
- COVID 19 Vaccine Development A Pediatric.20Document8 pagesCOVID 19 Vaccine Development A Pediatric.20Ashley RajivNo ratings yet
- Antimicrobial Resistance in ICUs An Update in The.2Document9 pagesAntimicrobial Resistance in ICUs An Update in The.2FIA SlotNo ratings yet
- Mec CronicaDocument29 pagesMec CronicaAlfredo Luis Arana MaqueraNo ratings yet
- Acute Kidney Injury in Interstitial Nephritis.5 PDFDocument7 pagesAcute Kidney Injury in Interstitial Nephritis.5 PDFFIA SlotNo ratings yet
- Tuberculous Meningitis: Where To From Here?: ReviewDocument8 pagesTuberculous Meningitis: Where To From Here?: ReviewGladys SuwantiNo ratings yet
- E057736 FullDocument8 pagesE057736 FullBladimir CentenoNo ratings yet
- Practice Modification For Pandemics: A Model For Surge Planning in ObstetricsDocument15 pagesPractice Modification For Pandemics: A Model For Surge Planning in ObstetricsJhuliana CabreraNo ratings yet
- Update On Antimalarials and Systemic Lupus Erythematosus: ReviewDocument11 pagesUpdate On Antimalarials and Systemic Lupus Erythematosus: ReviewVerónica Duménez JofréNo ratings yet
- Distinguishing Fungal and Bacterial Keratitis On Clinical Signs PDFDocument2 pagesDistinguishing Fungal and Bacterial Keratitis On Clinical Signs PDFJennifer ChávezNo ratings yet
- The Glutamine Debate in Surgery and Critical CareDocument7 pagesThe Glutamine Debate in Surgery and Critical CareDiana MonRoy PérezNo ratings yet
- Effectiveness of Kumquat Decoction For The Improvement of Cough Caused by SARS-CoV-2 Omicron Variants, A Multicentre, Prospective Observational StudyDocument8 pagesEffectiveness of Kumquat Decoction For The Improvement of Cough Caused by SARS-CoV-2 Omicron Variants, A Multicentre, Prospective Observational StudyCatherina MoszkowiczNo ratings yet
- COVID 19 A Review.1Document10 pagesCOVID 19 A Review.1Mohamed AlamariNo ratings yet
- Hysteroscopy in COVID-19 TimesDocument5 pagesHysteroscopy in COVID-19 TimesHernan PettorossiNo ratings yet
- Chik ChlidrenDocument6 pagesChik ChlidrenAlejandraSevillaNo ratings yet
- Estimating UV-C Sterilization Dosage For COVID-19 Pandemic Mitigation EffortsDocument4 pagesEstimating UV-C Sterilization Dosage For COVID-19 Pandemic Mitigation Effortschirag vyasNo ratings yet
- Continuum 2020Document21 pagesContinuum 2020Allan Salmeron100% (1)
- Effect of The COVID 19 Pandemic On Laboratory And.16Document4 pagesEffect of The COVID 19 Pandemic On Laboratory And.16Daniela Mihaela ConstantinNo ratings yet
- Opth 236571 A Review of The Differential Diagnosis of Acute Infectious CDocument9 pagesOpth 236571 A Review of The Differential Diagnosis of Acute Infectious CSonia Capirosi AyuningtiasNo ratings yet
- Virucidal Benefits of Povidone-Iodine Use On The Ocular Surface: A ReviewDocument6 pagesVirucidal Benefits of Povidone-Iodine Use On The Ocular Surface: A ReviewHerlinda ChalistyaNo ratings yet
- Navigating The Pandemic Response Life Cycle: Molecular Diagnostics and Immunoassays in The Context of COVID-19 ManagementDocument19 pagesNavigating The Pandemic Response Life Cycle: Molecular Diagnostics and Immunoassays in The Context of COVID-19 ManagementdebasreenitaNo ratings yet
- Ocular Tuberculosis: Position Paper On Diagnosis and Treatment ManagementDocument8 pagesOcular Tuberculosis: Position Paper On Diagnosis and Treatment ManagementTammy VaniaNo ratings yet
- An Update On Antiviral Therapy Against Sars-Cov-2: How Far Have We Come?Document15 pagesAn Update On Antiviral Therapy Against Sars-Cov-2: How Far Have We Come?RAVI KUMAR AkulaNo ratings yet
- Treatment of Coronavirus Disease 2019.4Document5 pagesTreatment of Coronavirus Disease 2019.4Gaby VillasmilNo ratings yet
- The Impact of Infectious Diseases Consultation On.4Document7 pagesThe Impact of Infectious Diseases Consultation On.4Jolohiño DíazNo ratings yet
- Tuberculosis in Children: Screening, Diagnosis and ManagementDocument10 pagesTuberculosis in Children: Screening, Diagnosis and ManagementSatria Bayu PratamaNo ratings yet
- Indirect Calorimetry in Critical Illness A New.3Document10 pagesIndirect Calorimetry in Critical Illness A New.3gjk5q24qrqNo ratings yet
- Ef Ficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-AnalysisDocument11 pagesEf Ficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-AnalysisCRS1973No ratings yet
- Endoscopy Guidline in Covid 19 EraDocument6 pagesEndoscopy Guidline in Covid 19 EraAmik IndrayaniNo ratings yet
- Ocular Manifestations of Bartonellosis: ReviewDocument6 pagesOcular Manifestations of Bartonellosis: ReviewNadhila IchwanNo ratings yet
- Neurocysticercosis An Update On Diagnosis,.10Document9 pagesNeurocysticercosis An Update On Diagnosis,.10RENZO ALEJANDRO ACUÑA FLORESNo ratings yet
- Febrile Seizures Emergency Medicine Perspective.5Document6 pagesFebrile Seizures Emergency Medicine Perspective.5ArseniNo ratings yet
- 2020.08.07 C19 - Nullane Salus Extra EcclesiamDocument2 pages2020.08.07 C19 - Nullane Salus Extra Ecclesiamragod2No ratings yet
- "Diagnosis Protocols and Case Management of Leptospirosis": Muhammad Hussein Gasem, MD Dr. Kariadi HospitalDocument10 pages"Diagnosis Protocols and Case Management of Leptospirosis": Muhammad Hussein Gasem, MD Dr. Kariadi HospitalSelfie C RijalNo ratings yet
- Diagnostic Implications of Salivary Biomarkers In.28Document10 pagesDiagnostic Implications of Salivary Biomarkers In.28Rohit ShahNo ratings yet
- Ruiz-Vega 2021 J. Phys. Photonics 3 011002Document9 pagesRuiz-Vega 2021 J. Phys. Photonics 3 011002Tadiwanashe ChitsvaNo ratings yet
- FLCCC Summary of The Evidence of Ivermectin in COVID 19Document3 pagesFLCCC Summary of The Evidence of Ivermectin in COVID 19Muhamad ZaidNo ratings yet
- Current State of Noninvasive, Continuous.12 PDFDocument7 pagesCurrent State of Noninvasive, Continuous.12 PDFFIA SlotNo ratings yet
- Summary of The Evidence For Ivermectin in COVID-19Document3 pagesSummary of The Evidence For Ivermectin in COVID-19Kent CheeNo ratings yet
- ICU-acquired Pneumonia: Is It Time To Use This Term?: EditorialDocument2 pagesICU-acquired Pneumonia: Is It Time To Use This Term?: EditorialkenniNo ratings yet
- HC610-00-UK BALLARD Mini-BAL SelectedEvidenceBooklet COPY-05459 2021Document20 pagesHC610-00-UK BALLARD Mini-BAL SelectedEvidenceBooklet COPY-05459 2021Popescu ValiNo ratings yet
- The High Risk Patient For Ambulatory Surgery.4Document8 pagesThe High Risk Patient For Ambulatory Surgery.4FIA SlotNo ratings yet
- Nutraceuticals For CovidDocument27 pagesNutraceuticals For CovidFatma BaysalNo ratings yet
- Update59 COVID 19 Therapeutics 1Document16 pagesUpdate59 COVID 19 Therapeutics 1Hendi PrihatnaNo ratings yet
- Stewardship Intervention To Optimize Central.1Document8 pagesStewardship Intervention To Optimize Central.1alergo.ramirezNo ratings yet
- 10 1097@MCC 0000000000000756Document8 pages10 1097@MCC 0000000000000756Ysik KbreraNo ratings yet
- The Association of Vaccination and The Incidence of New Cases of COVID-19 Among Health Care Workers, December 16, 2020, Through May 4, 2021Document6 pagesThe Association of Vaccination and The Incidence of New Cases of COVID-19 Among Health Care Workers, December 16, 2020, Through May 4, 2021Obsgyn UKI 9 Aug - 14 Okt 21No ratings yet
- Koroonameetmete MõjuDocument15 pagesKoroonameetmete MõjuRoger TammNo ratings yet
- Contoh Jurnal PromkesDocument15 pagesContoh Jurnal Promkeshusna arwaNo ratings yet
- BMJ 2021 068302.fullDocument15 pagesBMJ 2021 068302.fullFarid RzNo ratings yet
- Pathogenesis of Myeloproliferative NeoplasmsDocument17 pagesPathogenesis of Myeloproliferative NeoplasmsIsmi RachmanNo ratings yet
- Amjnsp 2014 36 51Document18 pagesAmjnsp 2014 36 51Ismi RachmanNo ratings yet
- The 2016 WHO Classification andDocument11 pagesThe 2016 WHO Classification andIsmi RachmanNo ratings yet
- Laboratory Investigation of Myeloproliferative NeoplasmsDocument15 pagesLaboratory Investigation of Myeloproliferative NeoplasmsIsmi RachmanNo ratings yet
- Hyperuricemia MeN PDFDocument4 pagesHyperuricemia MeN PDFIsmi RachmanNo ratings yet
- LAPORAN KASUS, Cerebral Venous Sinus Thrombosis, Myeloproliferative Disorder, Intracerebral HemorrhageDocument12 pagesLAPORAN KASUS, Cerebral Venous Sinus Thrombosis, Myeloproliferative Disorder, Intracerebral HemorrhageIsmi RachmanNo ratings yet
- Hyperuricemia MeN PDFDocument4 pagesHyperuricemia MeN PDFIsmi RachmanNo ratings yet
- Medicine: Rhabdomyolysis Following Status Epilepticus With HyperuricemiaDocument3 pagesMedicine: Rhabdomyolysis Following Status Epilepticus With HyperuricemiaIsmi RachmanNo ratings yet
- Hyperuricemia and Acute Kidney Injury Secondary To Spontaneous Tumor Lysis Syndrome in Low Risk Myelodysplastic SyndromeDocument4 pagesHyperuricemia and Acute Kidney Injury Secondary To Spontaneous Tumor Lysis Syndrome in Low Risk Myelodysplastic SyndromeIsmi RachmanNo ratings yet
- Case Report On Hyperuricemia Presenting As One-Sided DiseaseDocument7 pagesCase Report On Hyperuricemia Presenting As One-Sided DiseaseIsmi RachmanNo ratings yet
- Hyperuricemia in 2 Patients Receiving PalbociclibDocument2 pagesHyperuricemia in 2 Patients Receiving PalbociclibIsmi RachmanNo ratings yet
- Approach To A Case of Hyperuricemia: Singh V, Gomez VV, Swamy SGDocument7 pagesApproach To A Case of Hyperuricemia: Singh V, Gomez VV, Swamy SGsharu4291No ratings yet
- Bacaan 2 PDFDocument9 pagesBacaan 2 PDFIsmi RachmanNo ratings yet
- A. Obesity Is A Huge Problem in Many Western Countries and One Which NowDocument6 pagesA. Obesity Is A Huge Problem in Many Western Countries and One Which NowĐỗ Thị Thuý NgaNo ratings yet
- Osce History Taking Evaluation Form 2022Document1 pageOsce History Taking Evaluation Form 2022Jill SunNo ratings yet
- The Powerful Impact of StressDocument19 pagesThe Powerful Impact of StressMichael Angelo SeñaNo ratings yet
- Complicaciones Mini ImplantesDocument12 pagesComplicaciones Mini ImplantesNuvia PardoNo ratings yet
- Simplified ACLS AlgorithmDocument1 pageSimplified ACLS AlgorithmBrianNo ratings yet
- 0529 Protocol Update 6.2.09 PDFDocument57 pages0529 Protocol Update 6.2.09 PDFTowhidulIslamNo ratings yet
- Language and Students With Mental RetardationDocument22 pagesLanguage and Students With Mental Retardationmat2489100% (4)
- COVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare ProfessionalsDocument3 pagesCOVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare Professionalsvarshasharma05No ratings yet
- Stock Opname 2022Document9 pagesStock Opname 2022laboratorium rsitNo ratings yet
- CIPD Mental Health & Wellbeing Briefing For Managers May 2020Document23 pagesCIPD Mental Health & Wellbeing Briefing For Managers May 2020bya*boNo ratings yet
- Antihypertensive Drugs - Classification and SynthesisDocument14 pagesAntihypertensive Drugs - Classification and SynthesisCường NguyễnNo ratings yet
- Module 3-4: Writing Argumentative Essay - Page - 1Document28 pagesModule 3-4: Writing Argumentative Essay - Page - 1Jan Den Saul DalanNo ratings yet
- Fetal Growth Restriction Acog 2013Document14 pagesFetal Growth Restriction Acog 2013germanNo ratings yet
- Introduction To PsychiatryDocument153 pagesIntroduction To Psychiatrybelayneh anteneh100% (1)
- Information MSQ KROK 2 Medicine 2007 2021 NEUROLOGYDocument92 pagesInformation MSQ KROK 2 Medicine 2007 2021 NEUROLOGYReshma Shaji PnsNo ratings yet
- ACG AchalasiaDocument12 pagesACG AchalasiaIndi SaragiNo ratings yet
- T.L.E - Hairdressing 10/written Test Third Quarter Name: - Section: - CP#Document2 pagesT.L.E - Hairdressing 10/written Test Third Quarter Name: - Section: - CP#Jake PeñanoNo ratings yet
- Ocupol D Drops and Ointment PDFDocument3 pagesOcupol D Drops and Ointment PDFAnushka ShresthaNo ratings yet
- Increased Intracranial PressureDocument10 pagesIncreased Intracranial Pressureapi-3822433100% (10)
- On The Wins of Love: Intensifying Proper Hygiene of Learners Through "Pmes (Proper Hygiene Makes Everyone Safe) Wins" ProgramDocument19 pagesOn The Wins of Love: Intensifying Proper Hygiene of Learners Through "Pmes (Proper Hygiene Makes Everyone Safe) Wins" ProgramClarissa DamayoNo ratings yet
- Region: Arum TriphyllumDocument3 pagesRegion: Arum TriphyllumKamalNo ratings yet
- Foundation Timetable 2017Document13 pagesFoundation Timetable 2017Wahida Amalin Ab RazakNo ratings yet
- Scoring Systems in Anesthesia and PACUDocument16 pagesScoring Systems in Anesthesia and PACUmissyaaaaNo ratings yet
- The Complete CBT Guide For Depression and Low MoodDocument642 pagesThe Complete CBT Guide For Depression and Low Moodalanbray115No ratings yet
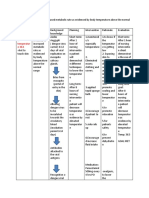
- NCP Dengue Fever Hyperthermia and Acute PainDocument4 pagesNCP Dengue Fever Hyperthermia and Acute PainJordz PlaciNo ratings yet
- Epilepsi 1Document12 pagesEpilepsi 1Ima SoniaNo ratings yet
- An Ethnobotanical Survey of Medicinal Plants Used in Terai Forest of Western NepalDocument15 pagesAn Ethnobotanical Survey of Medicinal Plants Used in Terai Forest of Western NepalLeandro DouglasNo ratings yet
- WD D-Healthy TravelerDocument6 pagesWD D-Healthy TravelercjNo ratings yet
- Clearance To Fly: Evidence of COVID Test AvailableDocument5 pagesClearance To Fly: Evidence of COVID Test AvailableSIM2004YA.RUNo ratings yet
- Science and Technology Grade 5 Term 2 Schemes of WorkDocument15 pagesScience and Technology Grade 5 Term 2 Schemes of Workmokuaben08No ratings yet