You might also like
- Metabolic Syndrome and Diabetes: A Bidirectional RelationshipDocument6 pagesMetabolic Syndrome and Diabetes: A Bidirectional RelationshipKarla MonsalvoNo ratings yet
- Nutrition and Alzheimer's Disease risk reductionDocument8 pagesNutrition and Alzheimer's Disease risk reductionPooja rameshNo ratings yet
- Insulin: Deficiency, Excess and Resistance in Human DiseaseFrom EverandInsulin: Deficiency, Excess and Resistance in Human DiseaseAndrew J. KrentzNo ratings yet
- Nutrigenomics and Cardiovascular DiseaseDocument19 pagesNutrigenomics and Cardiovascular DiseaseAssignmentLab.comNo ratings yet
- Mediterranean - Diet - Endothelial - Function - and - Vascular - Inflammatory - Markers 2018 PDFDocument4 pagesMediterranean - Diet - Endothelial - Function - and - Vascular - Inflammatory - Markers 2018 PDFPaulo CardosoNo ratings yet
- Physical Activity and Diabetes Prevention: Role of Exercise in Reducing The Risk of Diabetes and ObesityDocument9 pagesPhysical Activity and Diabetes Prevention: Role of Exercise in Reducing The Risk of Diabetes and ObesityMARLIA AGUSTINANo ratings yet
- Targeting Whole Body Metabolism and Mitochondrial Bioener - 2022 - Acta PharmaceDocument21 pagesTargeting Whole Body Metabolism and Mitochondrial Bioener - 2022 - Acta PharmaceMohammed Shuaib AhmedNo ratings yet
- Relationship of Fasting Plasma Adiponectin With Fasting Plasma Insulin in Young Non Diabetic IndividualsDocument9 pagesRelationship of Fasting Plasma Adiponectin With Fasting Plasma Insulin in Young Non Diabetic IndividualsIJAR JOURNALNo ratings yet
- Aguacate Gengibre ObesidadDocument9 pagesAguacate Gengibre ObesidadMike SánchezNo ratings yet
- Diabetes and Exercise: From Pathophysiology to Clinical ImplementationFrom EverandDiabetes and Exercise: From Pathophysiology to Clinical ImplementationJane E. B. Reusch, MDNo ratings yet
- Oral Antihyperglycemic Therapy For Type 2 Diabetes Mellitus: Review SynthèseDocument14 pagesOral Antihyperglycemic Therapy For Type 2 Diabetes Mellitus: Review SynthèseAlejandra GuiexubaNo ratings yet
- Association of Plasma Procalcitonin With Various Components of Metabolic Syndrome and Insulin ResistanceDocument13 pagesAssociation of Plasma Procalcitonin With Various Components of Metabolic Syndrome and Insulin ResistanceCentral Asian StudiesNo ratings yet
- Control GlicemicoDocument20 pagesControl GlicemicomiguelalmenarezNo ratings yet
- The Relationship of Plasma Adipsin Adiponectin VasDocument9 pagesThe Relationship of Plasma Adipsin Adiponectin VasRobert DwitamaNo ratings yet
- Journal Homepage: - : IntroductionDocument20 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Review Article: Functional Foods and Nutraceuticals in The Primary Prevention of Cardiovascular DiseasesDocument17 pagesReview Article: Functional Foods and Nutraceuticals in The Primary Prevention of Cardiovascular DiseasesUmar AliNo ratings yet
- Changes in Adiponectin Leptin RatioDocument7 pagesChanges in Adiponectin Leptin Ratioa12345644321No ratings yet
- Editorial The Role of Oxidative Stress in The Development of Diabetes Mellitus and Its ComplicationsDocument4 pagesEditorial The Role of Oxidative Stress in The Development of Diabetes Mellitus and Its Complicationsipd limabersaudaraNo ratings yet
- Management of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewDocument9 pagesManagement of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewsavitageraNo ratings yet
- Exercise-A:L-short Time-Obes Adult-2019-HeistonDocument10 pagesExercise-A:L-short Time-Obes Adult-2019-HeistonManaloe90No ratings yet
- Ketogenic Diets and Alzheimers DiseaseDocument9 pagesKetogenic Diets and Alzheimers DiseaseCaro GonzalezAFNo ratings yet
- Japplphysiol 00193 2005Document9 pagesJapplphysiol 00193 2005burhanNo ratings yet
- Paredes2013 - Cortisol The Villain in Metabolic SyndromeDocument9 pagesParedes2013 - Cortisol The Villain in Metabolic SyndromePaulo CesarNo ratings yet
- Gene-Diet Interactions in Complex DiseaseDocument9 pagesGene-Diet Interactions in Complex DiseaseJuan RocaNo ratings yet
- Sexual Dysfunction and The Mediterranean DietDocument3 pagesSexual Dysfunction and The Mediterranean DietAprilia MutiaraNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument7 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsGabriel GursenNo ratings yet
- Type 2 Diabetes The Lancet 2022Document18 pagesType 2 Diabetes The Lancet 2022Valentina Kerguelen HernándezNo ratings yet
- Adiponectin and Alzheimer's Disease: Is There A Link?: ReviewDocument7 pagesAdiponectin and Alzheimer's Disease: Is There A Link?: ReviewFritnerVélizNo ratings yet
- 1 s2.0 S0039128X13000901 MainDocument5 pages1 s2.0 S0039128X13000901 MainA NNo ratings yet
- Article: Dietary factors and diabetes-related health outcomes in patients with type 2 diabetes: protocol for a systematic review and meta-analysis of prospective observational studieDocument6 pagesArticle: Dietary factors and diabetes-related health outcomes in patients with type 2 diabetes: protocol for a systematic review and meta-analysis of prospective observational studieAndréia RochaNo ratings yet
- Archgenpsychiatry 2011 2Document8 pagesArchgenpsychiatry 2011 2ruba azfr-aliNo ratings yet
- Alimentos Hormonales, Experienciales y NeuronalesDocument7 pagesAlimentos Hormonales, Experienciales y NeuronalesJuanNo ratings yet
- 1 s2.0 S0002870320302143 MainDocument9 pages1 s2.0 S0002870320302143 MaindeepNo ratings yet
- Association Between Adiponectin and Atherosclerosis in RA PatientsDocument5 pagesAssociation Between Adiponectin and Atherosclerosis in RA PatientsIntan Winta PratiwiNo ratings yet
- Atherosclerosis: Contents Lists Available atDocument9 pagesAtherosclerosis: Contents Lists Available atAngelica Scherlowski FassulaNo ratings yet
- Lifestyle Modifications and Erectile Dysfunction: What Can Be Expected?Document6 pagesLifestyle Modifications and Erectile Dysfunction: What Can Be Expected?ANo ratings yet
- Association Between Diabetes Mellitus and Post Stroke Cognitive ImpairmentDocument6 pagesAssociation Between Diabetes Mellitus and Post Stroke Cognitive Impairmentvinnafazriharda3148No ratings yet
- Couple SMDocument11 pagesCouple SMbesti verawatiNo ratings yet
- tieuduongloai2Document16 pagestieuduongloai220128139No ratings yet
- A Deeper Dive Into Lipid Alterations in CKDDocument2 pagesA Deeper Dive Into Lipid Alterations in CKDAli TalalNo ratings yet
- Kefir Improves Blood Parameters and Reduces Cardiovascular Risks in Patients With Metabolic SyndromeDocument7 pagesKefir Improves Blood Parameters and Reduces Cardiovascular Risks in Patients With Metabolic SyndromeCristina OliveiraNo ratings yet
- Understanding Insulin in The Age of Precision Medicine and Big Data - Under-Explored Nature of GenomicsDocument38 pagesUnderstanding Insulin in The Age of Precision Medicine and Big Data - Under-Explored Nature of GenomicsGestne AureNo ratings yet
- Obesity Related Cognitive Impairment The Role of Endo - 2019 - Neurobiology ofDocument18 pagesObesity Related Cognitive Impairment The Role of Endo - 2019 - Neurobiology ofSabrina YenNo ratings yet
- Seminar: Epidemiology and Global Trends in Type 2 DiabetesDocument18 pagesSeminar: Epidemiology and Global Trends in Type 2 DiabetesRoopaNo ratings yet
- 2018 A Global Overview of Precision Medicine in Type 2 DiabetesDocument12 pages2018 A Global Overview of Precision Medicine in Type 2 Diabetesguanyulin01No ratings yet
- adiponectinDocument5 pagesadiponectinHaykal Estu BhismoroNo ratings yet
- From Genetic Risk Assessment To Diabetes Clinical InterventionDocument2 pagesFrom Genetic Risk Assessment To Diabetes Clinical InterventionBoo omNo ratings yet
- NIH Public AccessDocument23 pagesNIH Public AccesssiscupNo ratings yet
- NIH Public Access: The Road Connecting Obesity and Coronary Vasomotor Function: Straight Line or U-Turn?Document4 pagesNIH Public Access: The Road Connecting Obesity and Coronary Vasomotor Function: Straight Line or U-Turn?bawalNo ratings yet
- Metabolic Syndrome 2017 Diabetes Reversal by Plantbased Diet A Review Article Biswaroop Roy Chowdhury Indo Vietnam Medical BoardDocument2 pagesMetabolic Syndrome 2017 Diabetes Reversal by Plantbased Diet A Review Article Biswaroop Roy Chowdhury Indo Vietnam Medical Boardali shahidNo ratings yet
- GLX 041Document7 pagesGLX 041Tatta CamposNo ratings yet
- Research Paper On Diabetes Mellitus Type 2Document4 pagesResearch Paper On Diabetes Mellitus Type 2gvzrg8jy100% (1)
- Kun Lu CetakDocument15 pagesKun Lu CetakLYVXNo ratings yet
- Concurrent TrainingDocument12 pagesConcurrent Trainingfelipe diazNo ratings yet
- Literature Review On Type 2 Diabetes MellitusDocument7 pagesLiterature Review On Type 2 Diabetes Mellituscmppcmwgf100% (1)
- HHS Public Access: Sarcopenic Obesity in Older Adults: Aetiology, Epidemiology and Treatment StrategiesDocument61 pagesHHS Public Access: Sarcopenic Obesity in Older Adults: Aetiology, Epidemiology and Treatment Strategiesalif bagusNo ratings yet
- Nutrigenomics and cardiovascular gene regulationDocument6 pagesNutrigenomics and cardiovascular gene regulationTrismegisteNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument5 pagesJournal of Diabetes and Its ComplicationsDaniel Enrique Madera LópezNo ratings yet
- The Retinoblastoma Tumor-Suppressor Gene, The Exception That Proves The RuleDocument11 pagesThe Retinoblastoma Tumor-Suppressor Gene, The Exception That Proves The RuleSanthiya KunasegaranNo ratings yet
- TP53 Mutations in Human Cancers: Origins, Consequences, and Clinical UseDocument17 pagesTP53 Mutations in Human Cancers: Origins, Consequences, and Clinical UseSanthiya KunasegaranNo ratings yet
- The Rb/E2F Pathway and Cancer: Joseph R. NevinsDocument6 pagesThe Rb/E2F Pathway and Cancer: Joseph R. NevinsSanthiya KunasegaranNo ratings yet
- Review Article: Recent Advances in p53 Research and Cancer TreatmentDocument8 pagesReview Article: Recent Advances in p53 Research and Cancer TreatmentSanthiya KunasegaranNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptSanthiya KunasegaranNo ratings yet
- 5FU metabolism and its role in cancer treatmentDocument3 pages5FU metabolism and its role in cancer treatmentSanthiya KunasegaranNo ratings yet
- HHS Public AccessDocument17 pagesHHS Public AccessSanthiya KunasegaranNo ratings yet
- PRB y Ciclo Celular PDFDocument8 pagesPRB y Ciclo Celular PDFNacido para BendcirNo ratings yet
- Points For Question 2Document19 pagesPoints For Question 2Santhiya KunasegaranNo ratings yet
- Cronicon: Mini Review Cross Roads Between Insulin and Adiponectin Pathways: APPL1 PerspectiveDocument7 pagesCronicon: Mini Review Cross Roads Between Insulin and Adiponectin Pathways: APPL1 PerspectiveSanthiya KunasegaranNo ratings yet
- Points For Question 1Document30 pagesPoints For Question 1Santhiya KunasegaranNo ratings yet
- ReferencesDocument5 pagesReferencesSanthiya KunasegaranNo ratings yet
- Figure 1: The Common Mutation Sites in The Retinoblastoma Protein (PRB) - PRB Is Protein Made UpDocument8 pagesFigure 1: The Common Mutation Sites in The Retinoblastoma Protein (PRB) - PRB Is Protein Made UpSanthiya KunasegaranNo ratings yet
- MUNC-ing Around With Insulin Action: CommentariesDocument3 pagesMUNC-ing Around With Insulin Action: CommentariesSanthiya KunasegaranNo ratings yet
- Review Article: Role of Adiponectin in Central Nervous System DisordersDocument16 pagesReview Article: Role of Adiponectin in Central Nervous System DisordersSanthiya KunasegaranNo ratings yet
- Adiponectin, A Therapeutic Target For Obesity, Diabetes, and Endothelial DysfunctionDocument17 pagesAdiponectin, A Therapeutic Target For Obesity, Diabetes, and Endothelial DysfunctionJevon AndraNo ratings yet
- Adiponectin Signaling and Function in Insulin Target TissuesDocument9 pagesAdiponectin Signaling and Function in Insulin Target TissuesSanthiya KunasegaranNo ratings yet
- Large Intestine PDFDocument12 pagesLarge Intestine PDFSanthiya KunasegaranNo ratings yet
- TuitionDocument1 pageTuitionSanthiya KunasegaranNo ratings yet
- Mode of AssignmentDocument95 pagesMode of AssignmentQasim AliNo ratings yet
- Sika Poxitar FDocument3 pagesSika Poxitar FBudhi KurniawanNo ratings yet
- Grooved Peg BoardDocument2 pagesGrooved Peg BoarddanifgNo ratings yet
- Self Esteem and The Real Body ImageDocument12 pagesSelf Esteem and The Real Body ImageChy Alcarde50% (2)
- Physics Radiant Energy Light: GE 143 Remote SensingDocument1 pagePhysics Radiant Energy Light: GE 143 Remote SensingPISALBO, JEXTER P.No ratings yet
- Space suit essentialsDocument6 pagesSpace suit essentialsAdam PaiggeNo ratings yet
- Intermolecular Forces Lesson PlanDocument34 pagesIntermolecular Forces Lesson Planapi-442754652No ratings yet
- KJ's Take Out MenuDocument1 pageKJ's Take Out MenuintegiegirlNo ratings yet
- Cs Varnavrat Land SlideDocument7 pagesCs Varnavrat Land SlideBIJAY KRISHNA DASNo ratings yet
- Klubermatic Lubricant DispensersDocument13 pagesKlubermatic Lubricant Dispenserstatankise100% (1)
- 2) Coa-Vitamin-Dsm-Lot # XW91707139-146 PDFDocument16 pages2) Coa-Vitamin-Dsm-Lot # XW91707139-146 PDFNaeem AnjumNo ratings yet
- Adult Assessment: Head To Toe Assessment Is The Baseline and Ongoing Data That Is Needed OnDocument2 pagesAdult Assessment: Head To Toe Assessment Is The Baseline and Ongoing Data That Is Needed OnAldrin NavarroNo ratings yet
- People Magazine Ronnie Van Zant 4Document1 pagePeople Magazine Ronnie Van Zant 4Randy CarterNo ratings yet
- Unit 7. The Dynamics of Ecosystems.Document12 pagesUnit 7. The Dynamics of Ecosystems.nimolesaNo ratings yet
- APA Style Guide for Student PapersDocument24 pagesAPA Style Guide for Student PapersHeureuse MamanNo ratings yet
- Buller, Paul F. - Schuler, Randall S - Managing Organizations and People - Cases in Management, Organizational Behavior and Human Resource Management-Thomson - South-Western (2006)Document530 pagesBuller, Paul F. - Schuler, Randall S - Managing Organizations and People - Cases in Management, Organizational Behavior and Human Resource Management-Thomson - South-Western (2006)ezekiel capuzNo ratings yet
- PN Junction Formation and Barrier PotentialDocument9 pagesPN Junction Formation and Barrier PotentialchristlllNo ratings yet
- Biology 1Document4 pagesBiology 1yvonne villanuevaNo ratings yet
- RMO Orientation AIRMEDDocument130 pagesRMO Orientation AIRMEDqueenartemisNo ratings yet
- Syllabus of Modules FOR THE Electrician Domestic (ELE701)Document6 pagesSyllabus of Modules FOR THE Electrician Domestic (ELE701)udi969100% (1)
- Practical 5.17 Protein MaterialsDocument2 pagesPractical 5.17 Protein MaterialsdeeyamullaNo ratings yet
- Antibiotic Susceptibility TestDocument5 pagesAntibiotic Susceptibility Testfarhanna8100% (3)
- Onan RV GenSet Service ManualDocument136 pagesOnan RV GenSet Service ManualAlbert A Ghazaleh100% (2)
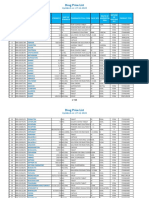
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- Sheath CurrentsDocument5 pagesSheath Currentsscribdkkk100% (1)
- Lab Report 2Document5 pagesLab Report 2adrianeNo ratings yet
- CompostAGuideForUsing PDFDocument4 pagesCompostAGuideForUsing PDFmkmikmiNo ratings yet
- Stabilizers: Agusta A W139 Maintenance Course Training ManualDocument6 pagesStabilizers: Agusta A W139 Maintenance Course Training ManualNita PuteriNo ratings yet
- Literature Review of ZnoDocument7 pagesLiterature Review of Znoea6mkqw2100% (1)
- 7Document40 pages7Felipe RichardiosNo ratings yet