You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Mushoku Tensei Volume 25 - Conclusion ChapterDocument73 pagesMushoku Tensei Volume 25 - Conclusion ChapterSeirei Est40% (5)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- LearningtoDrawPokemon NidoranFamilyDocument16 pagesLearningtoDrawPokemon NidoranFamilyLizzie Graham100% (2)
- Indice FacialDocument7 pagesIndice FacialAli ChaconNo ratings yet
- Rongga ObitaDocument27 pagesRongga ObitaFadli LatamaNo ratings yet
- OCC11 Q2 Mod7 Principles-of-Speech-Writing Version3 PDFDocument26 pagesOCC11 Q2 Mod7 Principles-of-Speech-Writing Version3 PDFKindred Binondo100% (10)
- Ortho4 Lec.8 Development of Occlusion (DR - Cube)Document39 pagesOrtho4 Lec.8 Development of Occlusion (DR - Cube)ahmednabaa230No ratings yet
- Rundown Rakernas & Seminar PABMI - Final-1Document6 pagesRundown Rakernas & Seminar PABMI - Final-1MarthinNo ratings yet
- Rhinoplasty: Septal Saddle Nose Deformity and Composite ReconstructionDocument15 pagesRhinoplasty: Septal Saddle Nose Deformity and Composite ReconstructionRosaMinnitiNo ratings yet
- MBT Brackets Placements TechniqueDocument10 pagesMBT Brackets Placements TechniqueTricky90100% (1)
- I Look in The MirrorDocument2 pagesI Look in The MirrorMohamad Azmi Mat NawiNo ratings yet
- Orthodontic Treatment of CLIII Malocclusions Using The Straight Wire ApplianceDocument8 pagesOrthodontic Treatment of CLIII Malocclusions Using The Straight Wire ApplianceCraciun TatianaNo ratings yet
- Cataract FinalDocument14 pagesCataract FinalSubha MaheswariNo ratings yet
- Removable Orthodontic Appliances - Jaypee Brothers (December 30, 2008) PDFDocument104 pagesRemovable Orthodontic Appliances - Jaypee Brothers (December 30, 2008) PDFRamon Mario De DonatisNo ratings yet
- Rims & Occlusal Record PDFDocument63 pagesRims & Occlusal Record PDFAmanda AmaroNo ratings yet
- Extraction Planningin OrthodonticsDocument6 pagesExtraction Planningin OrthodonticsAdina SerbanNo ratings yet
- Anterior Reference PointsDocument4 pagesAnterior Reference Pointsmadhusudhan udayagiriNo ratings yet
- Single Complete DentureDocument20 pagesSingle Complete DentureslidezbuzzNo ratings yet
- Full Anatomy CoassDocument74 pagesFull Anatomy CoassAuliaRusdiAllmuttaqienNo ratings yet
- Refraction by The EyeDocument28 pagesRefraction by The EyeCherry OrtegaNo ratings yet
- Face Recognition - Teacher's Notes: Warmer Activity (15-20 Min)Document5 pagesFace Recognition - Teacher's Notes: Warmer Activity (15-20 Min)Karina Cecilia Molina ArayaNo ratings yet
- Final c2 Summer 2017Document10 pagesFinal c2 Summer 2017Hassan TantawyNo ratings yet
- Lesson 3 - Basic Corrective MakeupDocument3 pagesLesson 3 - Basic Corrective Makeupethanjohannes100% (1)
- Benda Asing Dalam Kornea Akibat Kurangnya Peralatan Keselamatan: Laporan KasusDocument6 pagesBenda Asing Dalam Kornea Akibat Kurangnya Peralatan Keselamatan: Laporan KasusRachmad SammuliaNo ratings yet
- Oral Maxillofacial SurgeryDocument3 pagesOral Maxillofacial SurgeryR K100% (1)
- Face Recognition System Research PapersDocument8 pagesFace Recognition System Research Papersjhwmemrhf100% (1)
- Visual Outcomes Following Small Incision Cataract Surgery (SICS) in Wangaya HospitalDocument4 pagesVisual Outcomes Following Small Incision Cataract Surgery (SICS) in Wangaya HospitalKrisnhalianiNo ratings yet
- ORTHODONTIADocument10 pagesORTHODONTIArbNo ratings yet
- Guia de Odonto, Aplicado IVDocument3 pagesGuia de Odonto, Aplicado IVMaría Fernanda LariosNo ratings yet
- Dental Certificate FinalDocument2 pagesDental Certificate FinalRaquelito Belmonte Cenal100% (1)
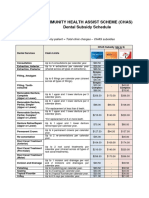
- CHAS Dental Subsidy ScheduleDocument1 pageCHAS Dental Subsidy ScheduleEugeneNo ratings yet