You might also like
- Fact Sheet: BiologicsDocument5 pagesFact Sheet: BiologicsJuan DiegoNo ratings yet
- Drugs Used in Pediatric DentistryDocument33 pagesDrugs Used in Pediatric Dentistryaamee9690% (10)
- Zinnat TabletsDocument5 pagesZinnat TabletsAndrei Marian BorcescuNo ratings yet
- TyphoidDocument2 pagesTyphoidFatma HasanNo ratings yet
- Dosing of Ivermectin & Other TherapeuticsDocument7 pagesDosing of Ivermectin & Other TherapeuticsTom100% (2)
- Antimicrobial Regiment Selection: Afifah Laboratorium Farmakologi Dan Terapi FK UnsoedDocument49 pagesAntimicrobial Regiment Selection: Afifah Laboratorium Farmakologi Dan Terapi FK Unsoed_sri_nurhayatiNo ratings yet
- Infliximab: Drug Treatment InformationDocument7 pagesInfliximab: Drug Treatment InformationAlin-Ionuț SălcianuNo ratings yet
- AntibioticGuidelines PrimaryDocument12 pagesAntibioticGuidelines PrimaryHandriyato SukmaNo ratings yet
- Emma Best, Simon Briggs, Rosemary Ikram, Mark Thomas - Antibiotics - Choices For Common Infections 2013 Edition (BPAC NZ) (2013, BPAC NZ)Document28 pagesEmma Best, Simon Briggs, Rosemary Ikram, Mark Thomas - Antibiotics - Choices For Common Infections 2013 Edition (BPAC NZ) (2013, BPAC NZ)igd rsudcpNo ratings yet
- Antibiotics Guide 2013Document30 pagesAntibiotics Guide 2013Stefani NoviliaNo ratings yet
- Antibiotics: Choices For Common InfectionsDocument30 pagesAntibiotics: Choices For Common InfectionsAlfeus GradyNo ratings yet
- Inflammatory Colitis - A RecapDocument34 pagesInflammatory Colitis - A RecapanahitaasharmaNo ratings yet
- Medication Fact Sheets: 3rd Edition ContributorsDocument50 pagesMedication Fact Sheets: 3rd Edition ContributorsIndumathi ThangathirupathiNo ratings yet
- Operation UeueueueDocument210 pagesOperation UeueueueBSRT1A BERBANO, IAN JEWEL M.No ratings yet
- Drugs Acting On The GitDocument29 pagesDrugs Acting On The GitIsheanesu MugwisiNo ratings yet
- Laboratory Diagnosis: 1. Cytological Examination (Tzanck Smear)Document11 pagesLaboratory Diagnosis: 1. Cytological Examination (Tzanck Smear)Rahma P T RambeyNo ratings yet
- "Magic Bullets": The AntibodiesDocument40 pages"Magic Bullets": The AntibodiesSherief AKNo ratings yet
- Denosumab-12mg Per 1.7ml Single Use Vial InjectionDocument10 pagesDenosumab-12mg Per 1.7ml Single Use Vial InjectionMd. Abdur RahmanNo ratings yet
- Guide Paed Bone JNTDocument11 pagesGuide Paed Bone JNTDorica GiurcaNo ratings yet
- STD PanelDocument10 pagesSTD PanelYateesh SrinivasaNo ratings yet
- What Is The Appendix?: Symptoms of AppendicitisDocument6 pagesWhat Is The Appendix?: Symptoms of AppendicitisVonn Bryan CalumiaNo ratings yet
- DiverticulitaDocument6 pagesDiverticulitaoxichinolinNo ratings yet
- Drug Study: PART 1: To Be Completed Prior To Clinical ExperienceDocument5 pagesDrug Study: PART 1: To Be Completed Prior To Clinical ExperienceFrozanSNo ratings yet
- Clinical Outcomes of Golimumab As First, Second or Third Anti-TNF Agent in Patients With Moderate-to-Severe Ulcerative ColitisDocument9 pagesClinical Outcomes of Golimumab As First, Second or Third Anti-TNF Agent in Patients With Moderate-to-Severe Ulcerative ColitisDiana GCNo ratings yet
- Drug StudyDocument10 pagesDrug StudybaniniycsebNo ratings yet
- Malaria 2012Document43 pagesMalaria 2012van_cristianoNo ratings yet
- Cefazolin (Ancef ®) : D5W, NsDocument9 pagesCefazolin (Ancef ®) : D5W, Nsbabe5606No ratings yet
- Kanamycin (Mode of Administration)Document3 pagesKanamycin (Mode of Administration)Waseem MaroofiNo ratings yet
- Client Profile Log Antenatal - CompleteDocument5 pagesClient Profile Log Antenatal - CompleteLinea GreeneNo ratings yet
- TyphoidDocument12 pagesTyphoidmansoorminahil149No ratings yet
- Artikel 1Document3 pagesArtikel 1Dieni Rhdezscpecjthor UnityNo ratings yet
- Enteral InfectionsDocument6 pagesEnteral InfectionsAshley CheungNo ratings yet
- Drug Study OrthoDocument17 pagesDrug Study OrthoMc Crister SilangNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- GavisconDocument8 pagesGavisconletisha mamaNo ratings yet
- PST OpDocument90 pagesPST OpBSRT1A BERBANO, IAN JEWEL M.No ratings yet
- Uworld Questions Nursing Nclex TestDocument292 pagesUworld Questions Nursing Nclex TestOlivia LowellNo ratings yet
- TB Guideline TreatmentDocument14 pagesTB Guideline TreatmentNovii NoviiNo ratings yet
- Modul PneumoniaDocument16 pagesModul Pneumoniaandamar0290No ratings yet
- Journal Reading: By: Vera Septia Nalurita (2008730129) Preceptor: Dr. Bowo Wahyudi, SPKK Rsud Kota BanjarDocument17 pagesJournal Reading: By: Vera Septia Nalurita (2008730129) Preceptor: Dr. Bowo Wahyudi, SPKK Rsud Kota BanjarVera Septia NaluritaNo ratings yet
- Zinnat PIDocument10 pagesZinnat PIfsdfNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Face Fracture Treatment & Management: Prehospital CareDocument7 pagesFace Fracture Treatment & Management: Prehospital Caremafoel39No ratings yet
- Adalizumab PDFDocument12 pagesAdalizumab PDFAyu Angger PuteriNo ratings yet
- InfectionDocument143 pagesInfectionMaria KamalNo ratings yet
- Drug StudyDocument7 pagesDrug StudyJuliana LegarteNo ratings yet
- Other Antiemetic Medications: Other 5HT3 Receptor AntagonistsDocument4 pagesOther Antiemetic Medications: Other 5HT3 Receptor AntagonistsYayaNo ratings yet
- TriclabendazolDocument1 pageTriclabendazolSílvia FanicaNo ratings yet
- Recommended Doses of IVERMECTINDocument3 pagesRecommended Doses of IVERMECTINRonald LunasNo ratings yet
- Management of Reactions in Leprosy: How Should Lepra Reactions Be Managed?Document2 pagesManagement of Reactions in Leprosy: How Should Lepra Reactions Be Managed?Echa AdityaNo ratings yet
- Anti Tubercular AgentsDocument22 pagesAnti Tubercular AgentsKakai Ablanque LopozNo ratings yet
- NCP and DrugsDocument7 pagesNCP and DrugsRach AbsalonNo ratings yet
- FDA Categorize Cyclophosphamide As PREGNANCY CATEGORY DDocument4 pagesFDA Categorize Cyclophosphamide As PREGNANCY CATEGORY DShane PangilinanNo ratings yet
- Dosage: Pediatric PatientsDocument4 pagesDosage: Pediatric PatientsanindythaNo ratings yet
- Antiviral Drugs Group 3 FinalDocument10 pagesAntiviral Drugs Group 3 FinalSpeed SamNo ratings yet
- Antibody Deficiency: Manchester Royal InfirmaryDocument8 pagesAntibody Deficiency: Manchester Royal Infirmaryfian silviakrisnasariNo ratings yet
- Tetanus Treatment & Management - Approach Considerations, Initial Supportive Therapy and Wound Care, Pharmacologic TherapyDocument11 pagesTetanus Treatment & Management - Approach Considerations, Initial Supportive Therapy and Wound Care, Pharmacologic TherapyFuad Adi PrasetyoNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
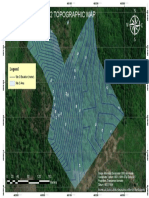
- Topographic Map2Document1 pageTopographic Map2AldiarsoNo ratings yet
- Bali 10 Year Load ForecastDocument1 pageBali 10 Year Load ForecastAldiarsoNo ratings yet
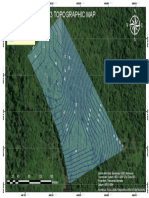
- Topographic Map3Document1 pageTopographic Map3AldiarsoNo ratings yet
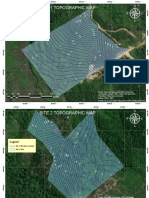
- PLTS Grogot Site Topographic MapDocument3 pagesPLTS Grogot Site Topographic MapAldiarsoNo ratings yet
- 3 - (2018) Characterizing Heat Stress On Livestock Using The Temperature Humidity IndexDocument12 pages3 - (2018) Characterizing Heat Stress On Livestock Using The Temperature Humidity IndexAldiarsoNo ratings yet
- 2 - (2012) Effect of Temperature-Humidity Index On Live Performance in BroilerDocument11 pages2 - (2012) Effect of Temperature-Humidity Index On Live Performance in BroilerAldiarsoNo ratings yet
- Air Cond Operation Manual SED - SMDDocument28 pagesAir Cond Operation Manual SED - SMDBimoNo ratings yet
- 1 - (2017) Review Control StrategyDocument28 pages1 - (2017) Review Control StrategyAldiarsoNo ratings yet
- 5 - (2017) Ind The Toolkit of Success Rate Calculation of Broiler HarvestDocument9 pages5 - (2017) Ind The Toolkit of Success Rate Calculation of Broiler HarvestAldiarsoNo ratings yet
- Laporan OtospectorDocument11 pagesLaporan OtospectorAldiarsoNo ratings yet
- Pennac-2 1 PDFDocument46 pagesPennac-2 1 PDFAldiarsoNo ratings yet
- App 1 Surayala FuelDocument15 pagesApp 1 Surayala FuelAldiarsoNo ratings yet
- Coal Beneficiation Technology 2007-Satyamurty PDFDocument21 pagesCoal Beneficiation Technology 2007-Satyamurty PDFxaver lawNo ratings yet
- Coal Beneficiation Technology 2007-Satyamurty PDFDocument21 pagesCoal Beneficiation Technology 2007-Satyamurty PDFxaver lawNo ratings yet
- Captive Breeding of The Spiny Lobster Panulirus Homarus PDFDocument11 pagesCaptive Breeding of The Spiny Lobster Panulirus Homarus PDFAldiarsoNo ratings yet
- 13Document65 pages13Ratti PrudhviNo ratings yet
- Alprazolam XanaxDocument2 pagesAlprazolam XanaxKristi WrayNo ratings yet
- History of PharmacyDocument8 pagesHistory of PharmacyHello50% (2)
- Drug NorvascDocument1 pageDrug NorvascSrkocherNo ratings yet
- Ibrufin EstimationDocument23 pagesIbrufin EstimationAnonymous XuiUo2ThNo ratings yet
- Antidote List 2 2011 PDFDocument12 pagesAntidote List 2 2011 PDFRiZqi RufiNo ratings yet
- Arylcyclohexamines (Ketamine, Phencyclidine, and Analogues)Document47 pagesArylcyclohexamines (Ketamine, Phencyclidine, and Analogues)gigidurul1111100% (1)
- 6 135Document6 pages6 135Ashok LenkaNo ratings yet
- SJC UzpharmsanoatDocument12 pagesSJC UzpharmsanoatLVKonfederacijaNo ratings yet
- Neurotransmitters and Drugs ChartDocument6 pagesNeurotransmitters and Drugs ChartTammy Tam100% (5)
- Rapid Analysis of Genotoxic Nitrosamines by HPLC MS MSDocument3 pagesRapid Analysis of Genotoxic Nitrosamines by HPLC MS MSMarcio SchiavelliNo ratings yet
- Stock Opname April 2017Document11 pagesStock Opname April 2017farid akbarNo ratings yet
- Kantor1986 PDFDocument10 pagesKantor1986 PDFjafs190594No ratings yet
- 26805550dft SV and Pharmacy Bulk Packages For PN Aluminum Content LabelingDocument26 pages26805550dft SV and Pharmacy Bulk Packages For PN Aluminum Content LabelingTumma RamaraoNo ratings yet
- 68 - What Is Kratom 20 Jul 2020Document3 pages68 - What Is Kratom 20 Jul 2020Rizal DaudNo ratings yet
- Drug Delivery Inhalation BioequivalenceDocument12 pagesDrug Delivery Inhalation Bioequivalenceparinaferns0% (1)
- SP Awal Pareto A SP Senin 17 Feb 2020 KF CLMDocument172 pagesSP Awal Pareto A SP Senin 17 Feb 2020 KF CLMIis IstikomahNo ratings yet
- Cardiovascular Drugs: Dr. Hazha S. Ameen MSCDocument25 pagesCardiovascular Drugs: Dr. Hazha S. Ameen MSCAhmed MohamadNo ratings yet
- MethimazoleDocument5 pagesMethimazoleapi-300595323No ratings yet
- GATE 2000 Que PaperDocument10 pagesGATE 2000 Que PaperSHRIKANTNo ratings yet
- Science Behind ZiconotideDocument3 pagesScience Behind ZiconotideLawrence SiervoNo ratings yet
- Health - 19-02-06 MEDICAL CANNABIS PDFDocument104 pagesHealth - 19-02-06 MEDICAL CANNABIS PDFJamielyn DilidiliNo ratings yet
- Roquette Pharma Oral Dosage BROCHURE LYCATAB Pregelatinised Maize StarchDocument26 pagesRoquette Pharma Oral Dosage BROCHURE LYCATAB Pregelatinised Maize StarchRong ZhaoNo ratings yet
- CME Quiz 2019 Jan Issue 1Document3 pagesCME Quiz 2019 Jan Issue 1Basil al-hashaikehNo ratings yet
- Antimanic DrugsDocument9 pagesAntimanic DrugscradletalkNo ratings yet
- J. DAFTAR PUSTAKADocument6 pagesJ. DAFTAR PUSTAKADewiNo ratings yet
- Anda Paragraph-Iv Filings A Complete Review PDFDocument17 pagesAnda Paragraph-Iv Filings A Complete Review PDFanurag sharmaNo ratings yet
- Musa Paradisiaca L. and Musa Sapientum L.: A Phytochemical and Pharmacological ReviewDocument8 pagesMusa Paradisiaca L. and Musa Sapientum L.: A Phytochemical and Pharmacological ReviewDeviNo ratings yet
- Daftar Obat Norum/Look Alike Sound AlikeDocument3 pagesDaftar Obat Norum/Look Alike Sound Alikewidia annisaNo ratings yet
- Over The Counter DrugsDocument28 pagesOver The Counter DrugsManjusha KondepudiNo ratings yet