You might also like
- BSC PT - Inpatient PT Evaluation FormDocument1 pageBSC PT - Inpatient PT Evaluation Formrambabs369100% (1)
- Sparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFDocument61 pagesSparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFzelma.bennett128100% (47)
- OPPE-FPPE ToolkitDocument71 pagesOPPE-FPPE ToolkitHosi Pba100% (1)
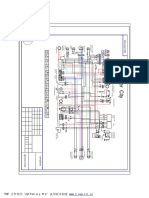
- Cpi Oliver City EldiagramDocument1 pageCpi Oliver City EldiagramHenry BraunNo ratings yet
- The Organic Farmer's Business Handbook by Richard Wiswall (Book Preview)Document26 pagesThe Organic Farmer's Business Handbook by Richard Wiswall (Book Preview)Chelsea Green Publishing100% (65)
- ECG Library PDFDocument98 pagesECG Library PDFJayden WaveNo ratings yet
- Ministry of Health Regulation No.736 Menkes Per VI 2010Document20 pagesMinistry of Health Regulation No.736 Menkes Per VI 2010krisna_esaNo ratings yet
- 997 Technical ManualDocument209 pages997 Technical Manualemmanuel geurtsNo ratings yet
- APTA Defensible DocumentationDocument3 pagesAPTA Defensible DocumentationEvaNo ratings yet
- Preview-90187 Pno H UnlockedDocument5 pagesPreview-90187 Pno H UnlockedFilip SuciuNo ratings yet
- Occupational Therapy Evaluation, Assessment and Treatment PlanDocument41 pagesOccupational Therapy Evaluation, Assessment and Treatment PlanPallavi BhatNo ratings yet
- BSC PT - European Standard of Physiotherapy PracticeDocument43 pagesBSC PT - European Standard of Physiotherapy Practicerambabs369No ratings yet
- Ppii Tutorial ManualDocument145 pagesPpii Tutorial ManualFabio BolivarNo ratings yet
- To Have and To Hold 8Document1 pageTo Have and To Hold 8Indra AristamaNo ratings yet
- Possible Artifacts For Danielson Domains 1 and 4Document4 pagesPossible Artifacts For Danielson Domains 1 and 4api-432851107100% (2)
- Agnus DeiDocument2 pagesAgnus DeiVoltaire ManzanoNo ratings yet
- Sanctus PDFDocument2 pagesSanctus PDFKe VinNo ratings yet
- Psalm - Second Sunday of Easter 2023Document1 pagePsalm - Second Sunday of Easter 2023Bienvenido Gipulao Santos Jr.No ratings yet
- 2016 (Vocal Score) AmenDocument1 page2016 (Vocal Score) AmenCultural SICNo ratings yet
- Compilation of SongsDocument587 pagesCompilation of SongsMarius PalafoxNo ratings yet
- One Bread One Body ChordsDocument2 pagesOne Bread One Body ChordspiedadmarkNo ratings yet
- It Took A CrossDocument2 pagesIt Took A CrossElla Marie Gamayon PoloNo ratings yet
- Holy, Holy, Holy PDFDocument1 pageHoly, Holy, Holy PDFJayveeMusicNo ratings yet
- Sherrygrandisonresume 2021Document7 pagesSherrygrandisonresume 2021api-577593865No ratings yet
- Lilley: Pharmacology and The Nursing Process, 7th EditionDocument8 pagesLilley: Pharmacology and The Nursing Process, 7th EditionthubtendrolmaNo ratings yet
- Sample Scholarship Thank You LetterDocument1 pageSample Scholarship Thank You LetterAngelica EganaNo ratings yet
- Pagkabighani-Score and PartsDocument4 pagesPagkabighani-Score and Partsjordz100% (1)
- Prove My Love (Original)Document1 pageProve My Love (Original)Jesse Wilson100% (3)
- The Lord Is My HopeDocument10 pagesThe Lord Is My HopeKing Reymel L. GonzalesNo ratings yet
- Sanctus: For CDC OnlyDocument2 pagesSanctus: For CDC OnlyJoegrey AguilarNo ratings yet
- Mass June 2021Document55 pagesMass June 2021Jun UrbanoNo ratings yet
- CM Eyes Has Not SeenDocument2 pagesCM Eyes Has Not Seenmcgrand9987No ratings yet
- Advantages of Voluntary Blood DonationDocument2 pagesAdvantages of Voluntary Blood DonationSarah Agudo FernandezNo ratings yet
- Sa Yo LamangDocument8 pagesSa Yo LamangJude BesingaNo ratings yet
- Worship SongsAs I Come Into Your Presence Past The Gates of Praise Into Your Sanctuary Till Were Standing Face To Face I Look Upon Your Countenance I See The Fullness of Your GraceDocument212 pagesWorship SongsAs I Come Into Your Presence Past The Gates of Praise Into Your Sanctuary Till Were Standing Face To Face I Look Upon Your Countenance I See The Fullness of Your GraceAmabelleMarceloNo ratings yet
- Documentation Patient Client Management APTADocument8 pagesDocumentation Patient Client Management APTAYahyaNo ratings yet
- Documentation, Patient, Client, AptaDocument10 pagesDocumentation, Patient, Client, AptaMarcos RiquelmeNo ratings yet
- Physical Therapy DocumentationDocument5 pagesPhysical Therapy Documentationamrutharam50% (2)
- Health and StandardDocument19 pagesHealth and StandardSA RAINo ratings yet
- The Standard And: ProceduresDocument19 pagesThe Standard And: ProceduresSA RAINo ratings yet
- OPPEDocument6 pagesOPPEbaetyNo ratings yet
- JCI Standards Interpretation - June12004Document18 pagesJCI Standards Interpretation - June12004Niharika SharmaNo ratings yet
- Materials/Equipment/Supplies: of ofDocument16 pagesMaterials/Equipment/Supplies: of ofSA RAINo ratings yet
- Critical Pathway: Clinical Pathways Have Four Main Components (Hill, 1994, Hill 1998)Document5 pagesCritical Pathway: Clinical Pathways Have Four Main Components (Hill, 1994, Hill 1998)pooja singhNo ratings yet
- Pasquale Esposito Antonio Dal Canton Author Information Article Notes Information Cited byDocument11 pagesPasquale Esposito Antonio Dal Canton Author Information Article Notes Information Cited byshoaib samNo ratings yet
- Chapter 2Document46 pagesChapter 2ulpa nur indahsari100% (2)
- SOAP NotesDocument28 pagesSOAP NotesVinayak SharmaNo ratings yet
- OPPE Dokter Di RS - EnglishDocument70 pagesOPPE Dokter Di RS - EnglishKetut Widiyasa BonaNo ratings yet
- Article: Employees Are Required To Complete An Annual AsDocument22 pagesArticle: Employees Are Required To Complete An Annual AsSA RAINo ratings yet
- Purpose/Objective: of ofDocument16 pagesPurpose/Objective: of ofSA RAINo ratings yet
- Possible Roles For PTs and PTAs During The Coronavirus PandemicDocument3 pagesPossible Roles For PTs and PTAs During The Coronavirus PandemiccassNo ratings yet
- Ethics Documents For Physio TherapistsDocument21 pagesEthics Documents For Physio TherapistsDeeksha JainNo ratings yet
- 1 What Is Clinical Audit v3Document6 pages1 What Is Clinical Audit v3dmshossain100% (1)
- DefensibleDocumentationElements PDFDocument2 pagesDefensibleDocumentationElements PDFdr_finch511No ratings yet
- Policies and Procedures On Conducting Initial Assessment Inefficient and Systematic MannerDocument9 pagesPolicies and Procedures On Conducting Initial Assessment Inefficient and Systematic MannerKari Kris Buenaflor Isanan100% (1)
- Nursing AuditDocument60 pagesNursing AuditValliammalShanmugam100% (9)
- Physical-Therapist As Patient ManagerDocument39 pagesPhysical-Therapist As Patient ManagerRomana VayaniNo ratings yet
- Organization Name Occupational Health Service: OrganizatitionaDocument16 pagesOrganization Name Occupational Health Service: OrganizatitionaSA RAINo ratings yet
- Clinical Audit ProtocolDocument14 pagesClinical Audit Protocolsami ketemaNo ratings yet
- Article: Sually Shed y Se VerDocument22 pagesArticle: Sually Shed y Se VerSA RAINo ratings yet
- Nursing DiagnosisDocument38 pagesNursing DiagnosisJR Rolf NeuqeletNo ratings yet
- Article: of ofDocument15 pagesArticle: of ofSA RAINo ratings yet
- Q-Solution 3 - 3Document44 pagesQ-Solution 3 - 3Eman ShalabyNo ratings yet
- Clinical Audit For Medical StudentsDocument6 pagesClinical Audit For Medical StudentsAmal SaeedNo ratings yet
- Audit How To Do Guide - May 2010Document12 pagesAudit How To Do Guide - May 2010LohJNo ratings yet
- Patient Client ManagementDocument8 pagesPatient Client ManagementMahiNo ratings yet
- BSC PT - General Physiotherapy Assessent FormDocument2 pagesBSC PT - General Physiotherapy Assessent Formrambabs3690% (1)
- BSC PT - Patient Consent Form For ClinicDocument2 pagesBSC PT - Patient Consent Form For Clinicrambabs369No ratings yet
- Check ListDocument1 pageCheck Listrambabs369No ratings yet
- Resume From Ramesh Babu ManivannanDocument14 pagesResume From Ramesh Babu Manivannanrambabs369No ratings yet
- Steps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-StepDocument9 pagesSteps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-Steprambabs369No ratings yet
- General Anatomy of The: Male Reproductive SystemDocument13 pagesGeneral Anatomy of The: Male Reproductive Systemrambabs369100% (1)
- Clinic BannerDocument1 pageClinic Bannerrambabs369No ratings yet
- Protein Elongation and Termination: Process Diagrams Step-by-StepDocument7 pagesProtein Elongation and Termination: Process Diagrams Step-by-Steprambabs369No ratings yet
- Intramembranous Ossification: Process Diagrams Step-by-StepDocument5 pagesIntramembranous Ossification: Process Diagrams Step-by-Steprambabs369No ratings yet
- Receptor-Mediated Endocytosis: Process Diagrams Step-by-StepDocument7 pagesReceptor-Mediated Endocytosis: Process Diagrams Step-by-Steprambabs369No ratings yet
- General Anatomy of The Immune SystemDocument29 pagesGeneral Anatomy of The Immune Systemrambabs369100% (2)
- Effects of Human Growth Hormone: Process Diagrams Step-by-StepDocument11 pagesEffects of Human Growth Hormone: Process Diagrams Step-by-Steprambabs369100% (1)
- The Sodium-Potassium Pump: Process Diagrams Step-by-StepDocument5 pagesThe Sodium-Potassium Pump: Process Diagrams Step-by-Steprambabs369No ratings yet
- How An Enzyme Works: Process Diagrams Step-by-StepDocument4 pagesHow An Enzyme Works: Process Diagrams Step-by-Steprambabs369No ratings yet
- Introductio To:: SplanchnologyDocument36 pagesIntroductio To:: Splanchnologyrambabs369No ratings yet
- ARTHOLOGYDocument38 pagesARTHOLOGYrambabs369No ratings yet
- Cell Division: Mitosis and Cytokinesis: Process Diagrams Step-by-StepDocument7 pagesCell Division: Mitosis and Cytokinesis: Process Diagrams Step-by-Steprambabs369No ratings yet
- Clinical Biochemistry Reference Ranges HandbookDocument20 pagesClinical Biochemistry Reference Ranges Handbookrambabs369No ratings yet
- Medical Imaging Course Syllabus - Magnetic Resonance Imaging and Spectroscopy 31 Oct-2 November 2011 Sutton Campus of The Royal Marsden Hospital and Institute of Cancer SyllabusDocument9 pagesMedical Imaging Course Syllabus - Magnetic Resonance Imaging and Spectroscopy 31 Oct-2 November 2011 Sutton Campus of The Royal Marsden Hospital and Institute of Cancer Syllabusrambabs369No ratings yet
- Introduction To OesteologyDocument86 pagesIntroduction To Oesteologyrambabs369No ratings yet
- BSC PT - Lumbosacral Physiotherapy Evaluation FormDocument2 pagesBSC PT - Lumbosacral Physiotherapy Evaluation Formrambabs369100% (1)
- Chapter One Introduction To PathologyDocument26 pagesChapter One Introduction To Pathologyrambabs369No ratings yet
- Unit 1 - Introduction To PsychologyDocument8 pagesUnit 1 - Introduction To Psychologyrambabs369No ratings yet
- Time Off SlipDocument1 pageTime Off Sliprambabs369No ratings yet
- PHD Usa UnivDocument1 pagePHD Usa Univrambabs369No ratings yet
- Student Name List Sem I&IIDocument2 pagesStudent Name List Sem I&IIrambabs369No ratings yet
- Lecture-1 Introduction To Power Generation and Electrical Power SystemsDocument30 pagesLecture-1 Introduction To Power Generation and Electrical Power SystemsArishaNo ratings yet
- 14 StatisticsDocument15 pages14 StatisticsDROZON GAMING YTNo ratings yet
- Nasib Ahmad Faqirzada Resume CVDocument4 pagesNasib Ahmad Faqirzada Resume CVNasib Ahmad FaqirzadaNo ratings yet
- Phontech Ics 6200Document193 pagesPhontech Ics 6200danh voNo ratings yet
- Lunch With AbbreviationsDocument2 pagesLunch With AbbreviationsthefallsteamNo ratings yet
- Jsa For Inst. of TSF & Laydown AreaDocument23 pagesJsa For Inst. of TSF & Laydown AreaAshir RIZNo ratings yet
- NCSS Questions: Lte Ra Pao 3.0Document38 pagesNCSS Questions: Lte Ra Pao 3.0Imran AslamNo ratings yet
- Part 4 Experiments4Document12 pagesPart 4 Experiments4XI - TITL 121M. Bagas Sandika PratamaNo ratings yet
- CVDocument1 pageCVSiddharth ChauhanNo ratings yet
- 09-S and P Block Elements - Set-Test-Final-EDocument3 pages09-S and P Block Elements - Set-Test-Final-EAbhishek RavirajNo ratings yet
- 6 Storm Water Master SpreadsheetDocument16 pages6 Storm Water Master Spreadsheetscelo butheleziNo ratings yet
- Gabriela F. Sullivan: EducationDocument1 pageGabriela F. Sullivan: Educationapi-437973487No ratings yet
- Energy IndustriesDocument26 pagesEnergy IndustriesoliverphysicsNo ratings yet
- Religious Freedom: Why Now? Defending An Embattled Human RightDocument97 pagesReligious Freedom: Why Now? Defending An Embattled Human RightIslam and Religious Freedom100% (2)
- DexX A Double Layer Unpacking Framework For AndroidDocument10 pagesDexX A Double Layer Unpacking Framework For Androidali saaedNo ratings yet
- The LEGO Adventure BookDocument194 pagesThe LEGO Adventure BookBenjamin De AlexandrisNo ratings yet
- Being and Nothingness The Look SartreDocument3 pagesBeing and Nothingness The Look Sartremaximomore50% (4)
- Draft 2Document7 pagesDraft 2api-446158134No ratings yet
- Home-Made Cooking: Homemade Food Saves MoneyDocument2 pagesHome-Made Cooking: Homemade Food Saves MoneyDamaris ZlatanNo ratings yet
- GMORS Rubber Especification O Rings Guidebook AS568ADocument90 pagesGMORS Rubber Especification O Rings Guidebook AS568AfeltofsnakeNo ratings yet
- VSC Product Introduction-EnDocument36 pagesVSC Product Introduction-EnAldeni Prima AnugrahNo ratings yet
- GearsDocument246 pagesGearsVinayak AryanNo ratings yet
- Gaston BuffedDocument5 pagesGaston BuffedtimNo ratings yet
- Wa0001Document1 pageWa0001Boru RajaNo ratings yet
- Anime Neon Vibes Marketing PlanDocument62 pagesAnime Neon Vibes Marketing PlanAL - HusainNo ratings yet
- Use of Nonaqueous Solvents in Parenteral ProductsDocument11 pagesUse of Nonaqueous Solvents in Parenteral ProductsMustafa ShahinNo ratings yet