You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- An Adult With Childhood Medical Trauma Treated With Psychoanalytic Psychotherapy and EMDR: A Case StudyDocument11 pagesAn Adult With Childhood Medical Trauma Treated With Psychoanalytic Psychotherapy and EMDR: A Case StudyJuan Andres EspinozaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Maintenance and Operation Manual: Ultra Flow Type 'E-Fc' Gate ValvesDocument32 pagesMaintenance and Operation Manual: Ultra Flow Type 'E-Fc' Gate ValvesNeilton Junior100% (2)
- Supracondylar Fracture of The HumerusDocument19 pagesSupracondylar Fracture of The HumerusMai HunnyNo ratings yet
- 2017 Book ComplicationsOfTemporomandibul PDFDocument178 pages2017 Book ComplicationsOfTemporomandibul PDFJuan Andres EspinozaNo ratings yet
- Reliance Mud Pump Expendables Catalog PDFDocument17 pagesReliance Mud Pump Expendables Catalog PDFhebert perez100% (1)
- Save Electricity at WorkDocument16 pagesSave Electricity at WorkRaison MukkathNo ratings yet
- Dental Caries An Update Medical Model Risk AssesmentDocument6 pagesDental Caries An Update Medical Model Risk AssesmentJuan Andres EspinozaNo ratings yet
- Caries Risk Assessment A Systematic ReviewDocument12 pagesCaries Risk Assessment A Systematic ReviewJuan Andres EspinozaNo ratings yet
- Evaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss A Systematic Review and Meta-AnalysisDocument9 pagesEvaluation of Cement-Retained Versus Screw-Retained Implant-Supported Restorations For Marginal Bone Loss A Systematic Review and Meta-AnalysisJuan Andres EspinozaNo ratings yet
- Branemark 2003 Concepto All4Document8 pagesBranemark 2003 Concepto All4Juan Andres EspinozaNo ratings yet
- Cementar Zirconia Con Cemento Tto de Superficie PDFDocument10 pagesCementar Zirconia Con Cemento Tto de Superficie PDFJuan Andres EspinozaNo ratings yet
- Diseño de Apoyos en Dad CamDocument3 pagesDiseño de Apoyos en Dad CamJuan Andres EspinozaNo ratings yet
- Knowledge of Pregnant Women About Pregnancy Gingivitis and Children Oral HealthDocument10 pagesKnowledge of Pregnant Women About Pregnancy Gingivitis and Children Oral HealthJuan Andres EspinozaNo ratings yet
- Apoyos Elementos FinitosDocument7 pagesApoyos Elementos FinitosJuan Andres EspinozaNo ratings yet
- Efecto de La Funcion en Extension DistalDocument4 pagesEfecto de La Funcion en Extension DistalJuan Andres EspinozaNo ratings yet
- 3 Scaners Journal 2019 PDFDocument8 pages3 Scaners Journal 2019 PDFJuan Andres EspinozaNo ratings yet
- Cocrane PDFDocument19 pagesCocrane PDFJuan Andres EspinozaNo ratings yet
- Medical Provider Promotion of Oral Health and Women's Receipt of Dental Care During PregnancyDocument13 pagesMedical Provider Promotion of Oral Health and Women's Receipt of Dental Care During PregnancyJuan Andres EspinozaNo ratings yet
- Articulo3 PDFDocument8 pagesArticulo3 PDFJuan Andres EspinozaNo ratings yet
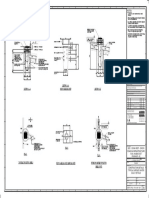
- Notes:: - DW016 ATK SW 7201 P02Document1 pageNotes:: - DW016 ATK SW 7201 P02Balaji NaikNo ratings yet
- Cisco SR2016 16-PortDocument3 pagesCisco SR2016 16-PortLuqman HakimNo ratings yet
- Electricity: One Mark QuestionsDocument26 pagesElectricity: One Mark Questionsashok pradhanNo ratings yet
- Buku ForkliftDocument192 pagesBuku ForkliftsatriyobcNo ratings yet
- Chapter 4: Functional Anatomy of Prokaryotic and Eukaryotic CellsDocument94 pagesChapter 4: Functional Anatomy of Prokaryotic and Eukaryotic CellsTrevannie EdwardsNo ratings yet
- Chemotherapy Class NoteDocument112 pagesChemotherapy Class Noteshrey patelNo ratings yet
- Green Your Block Tree Guard ApplicationDocument9 pagesGreen Your Block Tree Guard ApplicationScott M. Stringer0% (1)
- Logarithms and Decibels PDFDocument6 pagesLogarithms and Decibels PDFSirine AjourNo ratings yet
- Flow TestDocument6 pagesFlow Testhfdshy12No ratings yet
- VANGLAINI June 23Document12 pagesVANGLAINI June 23Zoramsanga GuiteNo ratings yet
- Front PageDocument6 pagesFront PageNaga TejaNo ratings yet
- Skills in Clinical Nursing 8Th Edition Berman Test Bank Full Chapter PDFDocument17 pagesSkills in Clinical Nursing 8Th Edition Berman Test Bank Full Chapter PDFcarolyn.mullen927100% (16)
- Transmission LinesDocument60 pagesTransmission LinesChenette Ahorro FerrerNo ratings yet
- 3D BioprintingDocument8 pages3D BioprintingCarooNo ratings yet
- Pamphlet - BMBS - WagonsDocument4 pagesPamphlet - BMBS - WagonsRakesh JainwalNo ratings yet
- Welding of SteelDocument7 pagesWelding of SteelAlbert CostasNo ratings yet
- Pelvic Inflammatory Disease - Clinical Manifestations and DiagnosisDocument13 pagesPelvic Inflammatory Disease - Clinical Manifestations and DiagnosisJavier Manuel Escobedo CalderónNo ratings yet
- Business Ethics: Submited byDocument8 pagesBusiness Ethics: Submited byAwais RanaNo ratings yet
- Lasers & HolographyDocument12 pagesLasers & HolographySyed Muzammil AliNo ratings yet
- August-8-2022 - Micro Part 1Document20 pagesAugust-8-2022 - Micro Part 1JAYMEE ROSS CASANo ratings yet
- ACCT504 Case Study 1 The Complete AccounDocument16 pagesACCT504 Case Study 1 The Complete AccounAnik BhowmickNo ratings yet
- SPH 280 - Cell Data Sheet: ClassificationDocument2 pagesSPH 280 - Cell Data Sheet: ClassificationWilson PavãoNo ratings yet
- Hafren Cost Plan Report r1Document23 pagesHafren Cost Plan Report r1Armin StraussNo ratings yet
- Spanish CasserolesDocument50 pagesSpanish CasserolesCamilleNo ratings yet
- Validity: Mcgraw-Hill/Irwin © 2013 Mcgraw-Hill Companies. All Rights ReservedDocument15 pagesValidity: Mcgraw-Hill/Irwin © 2013 Mcgraw-Hill Companies. All Rights ReservedNurul Fatin HusnaNo ratings yet
- 2011 NLRC Rules of ProcedureDocument75 pages2011 NLRC Rules of ProcedureJ.N.No ratings yet