You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MCQSDocument6 pagesMCQSkhuzaima9100% (2)
- Daphnia Lab ReportDocument3 pagesDaphnia Lab ReportHaley Baas100% (3)
- Ass 1 Unit 26 16-17Document3 pagesAss 1 Unit 26 16-17Anonymous RzVl4YDC0% (1)
- CIPD CH L 5 Org Dev and Reward PDFDocument80 pagesCIPD CH L 5 Org Dev and Reward PDFDrShabbir Khan50% (2)
- An Introduction To Formal Languages and Automata 5th Edition Solution ManualDocument4 pagesAn Introduction To Formal Languages and Automata 5th Edition Solution ManualEvelyn RM25% (4)
- C496 PDFDocument4 pagesC496 PDFpraneethaNo ratings yet
- Personal Statement Guide by Doctor Laska PDFDocument3 pagesPersonal Statement Guide by Doctor Laska PDFSteve JohnsonNo ratings yet
- Oleander PoisoningDocument19 pagesOleander PoisoningAnbu Arasan100% (1)
- PKK Kanak-Kanak Berkeperluan KhasDocument11 pagesPKK Kanak-Kanak Berkeperluan Khassyisyirararoro100% (1)
- GgreDocument8 pagesGgreHamsterindNo ratings yet
- DLL Science-6 Q3 W6Document4 pagesDLL Science-6 Q3 W6juvelyn.aclaoNo ratings yet
- Environmental Systems and Societies Paper 2 SL MarkschemeDocument8 pagesEnvironmental Systems and Societies Paper 2 SL MarkschemeAfra LamisaNo ratings yet
- Airspan ASMAX Product Brochure (QuantumWimax - Com)Document20 pagesAirspan ASMAX Product Brochure (QuantumWimax - Com)Ari Zoldan100% (1)
- Resume - Vanessa ADocument2 pagesResume - Vanessa Aapi-438977556No ratings yet
- Data Warehouse: Bilal HussainDocument20 pagesData Warehouse: Bilal HussainDaneil RadcliffeNo ratings yet
- Manual Hc-V268e HC-V268E 60af8211029cbDocument49 pagesManual Hc-V268e HC-V268E 60af8211029cbRoland BokorNo ratings yet
- Product Requirements Document TemplateDocument8 pagesProduct Requirements Document TemplateJonathan Rizky100% (4)
- PPS Magnet Registration Deadline Extended To December 18Document2 pagesPPS Magnet Registration Deadline Extended To December 18Alex OsgoodNo ratings yet
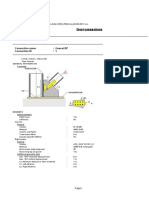
- Steel Connections: Detailed ReportDocument7 pagesSteel Connections: Detailed Reportgv Sathishkumar KumarNo ratings yet
- VCRCDocument75 pagesVCRCsunil SubaiNo ratings yet
- Synopsys DWDocument11 pagesSynopsys DWRanjit YewaleNo ratings yet
- CARTE-Politorbis Genocide Prevention FinalDocument158 pagesCARTE-Politorbis Genocide Prevention FinalV.N.INo ratings yet
- Heat Pump Training System Model 3402Document4 pagesHeat Pump Training System Model 3402Darwin SemanateNo ratings yet
- Good Hope School 13-18-1B Ch.9 Congruence Similarity CQDocument4 pagesGood Hope School 13-18-1B Ch.9 Congruence Similarity CQchristielam123No ratings yet
- Diffuse Sensor With Background Suppression: DesignDocument2 pagesDiffuse Sensor With Background Suppression: DesignhamidouhouNo ratings yet
- HYDRO-GUARD® Water-Based Drilling Fluid Delivering Stable Wellbore ThroughDocument1 pageHYDRO-GUARD® Water-Based Drilling Fluid Delivering Stable Wellbore ThroughFauzan Rahman HaqNo ratings yet
- Review 11 - Linking VerbsDocument1 pageReview 11 - Linking VerbsCindy TranNo ratings yet
- 34-Digital Marketing Assignment BriefDocument3 pages34-Digital Marketing Assignment BriefNabeel hassanNo ratings yet
- Recruitment and Selection in PIADocument2 pagesRecruitment and Selection in PIAAsad Khan100% (1)
- IntersubjectivityDocument32 pagesIntersubjectivityNashwaAlinsangaoNo ratings yet