You might also like
- Patient Progress Note ProtocolDocument8 pagesPatient Progress Note ProtocolVito Wilfredo100% (1)
- BBHF Ubot Wack0s Crack GuideDocument5 pagesBBHF Ubot Wack0s Crack GuideStephanie Wilson100% (1)
- 13 ElectronicHealthRecordDocument48 pages13 ElectronicHealthRecordkimchi girl100% (1)
- SOP For Procurement of Medical DevicesDocument2 pagesSOP For Procurement of Medical DevicesMuhammad Nisar50% (4)
- Health Record Documentation in Acute CareDocument8 pagesHealth Record Documentation in Acute Careapi-340699040No ratings yet
- 3rd Edition NABH Guidebook 2012.newDocument258 pages3rd Edition NABH Guidebook 2012.newDavid Turner93% (14)
- C++ Notes For Ignou StudentsDocument42 pagesC++ Notes For Ignou StudentsRamanpreet SinghNo ratings yet
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordFrom EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordNo ratings yet
- Deep C ModifiedDocument449 pagesDeep C ModifiedAmit DubeyNo ratings yet
- Admitting Clerk Job DescriptionDocument3 pagesAdmitting Clerk Job DescriptionMaria Edel100% (2)
- PrimeTime SlidesDocument47 pagesPrimeTime SlidesRamakrishnaRao SoogooriNo ratings yet
- Reaction PaperDocument1 pageReaction PaperSui Narcan100% (1)
- 01022E B61863E-13-5 SA1 SB7 Programming ManualDocument145 pages01022E B61863E-13-5 SA1 SB7 Programming Manualchinhctm100% (2)
- Clinical Evaluation Under EU MDR: Author - Dr. Amie Smirthwaite, Global VP For Clinical Services, RMQ+Document21 pagesClinical Evaluation Under EU MDR: Author - Dr. Amie Smirthwaite, Global VP For Clinical Services, RMQ+Doaa KhalilNo ratings yet
- Ebook 9 Steps It Audit ReadinessDocument28 pagesEbook 9 Steps It Audit ReadinessMarco Encina G.100% (1)
- Sectioning - Creating Unnumbered Chapters - Sections (Plus Adding Them To The ToC and - or Header) - TeX - LaTeX Stack ExchangeDocument3 pagesSectioning - Creating Unnumbered Chapters - Sections (Plus Adding Them To The ToC and - or Header) - TeX - LaTeX Stack ExchangeDeepak TaleleNo ratings yet
- REVISED IHOMP SAT v2 - For HospitalsDocument13 pagesREVISED IHOMP SAT v2 - For HospitalsMeme LangNo ratings yet
- Bladder Irrigation & InstallationDocument12 pagesBladder Irrigation & InstallationSui NarcanNo ratings yet
- The Insider's Guide To Network AutomationDocument11 pagesThe Insider's Guide To Network AutomationPreyasiMehtaNo ratings yet
- 13 ClinicalsummariesDocument2 pages13 Clinicalsummariesapi-101814919No ratings yet
- Rekam Medis ElektronikDocument3 pagesRekam Medis ElektronikDwi JokoNo ratings yet
- Test Procedure For 170.314 (B) (7) Data PortabilityDocument19 pagesTest Procedure For 170.314 (B) (7) Data PortabilitySpit FireNo ratings yet
- Test Procedure For 170.314 (B) (7) Data PortabilityDocument15 pagesTest Procedure For 170.314 (B) (7) Data PortabilitySpit FireNo ratings yet
- ONC Notice of Proposed Ruling Making Stage 2 Certification Rule Fact SheetDocument3 pagesONC Notice of Proposed Ruling Making Stage 2 Certification Rule Fact SheetEmilioCruzFernandezNo ratings yet
- FAQs 011922Document6 pagesFAQs 011922salyouhaNo ratings yet
- Diagnosis, and TherapiesDocument6 pagesDiagnosis, and TherapiesHoney MacabuhayNo ratings yet
- Medicare & Medicaid EHR Incentive Program: Meaningful Use Stage 1 Requirements OverviewDocument33 pagesMedicare & Medicaid EHR Incentive Program: Meaningful Use Stage 1 Requirements OverviewDodie DelosaNo ratings yet
- EHR Meaningful Use Guide PDFDocument24 pagesEHR Meaningful Use Guide PDFSpit FireNo ratings yet
- HL7 Meaningful Use - White PaperDocument5 pagesHL7 Meaningful Use - White Paperarijit00No ratings yet
- Standards For Outpatient Clinical ServicesDocument10 pagesStandards For Outpatient Clinical Servicessaintiyke58No ratings yet
- Assignment No 1-A SRSDocument6 pagesAssignment No 1-A SRSswatisahireNo ratings yet
- NX Info Reporting Dump PDFDocument11 pagesNX Info Reporting Dump PDFJar JeonNo ratings yet
- Costs and Limitations Disclosure For MEDITECH S 2014 Edition Certified Products PDFDocument9 pagesCosts and Limitations Disclosure For MEDITECH S 2014 Edition Certified Products PDFSpit FireNo ratings yet
- Benchbook Self Assessment Manual 1 ProtectedDocument77 pagesBenchbook Self Assessment Manual 1 ProtectedGeraldine Gallaron - CasipongNo ratings yet
- EBC EHAQ 4 Audit Tool Final January 2024Document46 pagesEBC EHAQ 4 Audit Tool Final January 2024AberaNo ratings yet
- Meaningful Use Stage 3 Recommendations - 2014!03!11Document17 pagesMeaningful Use Stage 3 Recommendations - 2014!03!11bgrabberNo ratings yet
- Test Bank For Electronic Health Records and Nursing 1st Edition Richard GarteeDocument21 pagesTest Bank For Electronic Health Records and Nursing 1st Edition Richard GarteeFrederick Jones100% (38)
- Onc Regulations Faqs: Question (9-10-001-1) : What Certification Criteria Will Onc-Atcbs Use To Certify EhrDocument20 pagesOnc Regulations Faqs: Question (9-10-001-1) : What Certification Criteria Will Onc-Atcbs Use To Certify EhrRich ElmoreNo ratings yet
- Issue Date: February 6, 2017: Accreditation Survey Activity Guide For Health Care OrganizationsDocument107 pagesIssue Date: February 6, 2017: Accreditation Survey Activity Guide For Health Care OrganizationsNYONGKERNo ratings yet
- What Do Employer's Want For Their Employees?: Standardization With IndividualizationDocument4 pagesWhat Do Employer's Want For Their Employees?: Standardization With Individualizationapi-304631562No ratings yet
- Software Requirement OPD ManagementDocument35 pagesSoftware Requirement OPD ManagementAnindam Basu71% (17)
- What Do Employer's Want For Their Employees?: Standardization With IndividualizationDocument4 pagesWhat Do Employer's Want For Their Employees?: Standardization With Individualizationapi-304631562No ratings yet
- Midterms - HA LabDocument17 pagesMidterms - HA LabMa. Daniela De la CernaNo ratings yet
- HA-Midterms LabDocument13 pagesHA-Midterms LabMa. Daniela De la CernaNo ratings yet
- Audit Checklist Non-CMSDocument7 pagesAudit Checklist Non-CMSsavvy_as_98-1No ratings yet
- Out Put 2Document47 pagesOut Put 2peter mulilaNo ratings yet
- Jds ST JohnsDocument57 pagesJds ST Johnspeter mulilaNo ratings yet
- Defensible Documentation Quick ReferenceDocument3 pagesDefensible Documentation Quick ReferencecderdnaseNo ratings yet
- Test Bank For Electronic Health Records and Nursing 1st Edition Richard GarteeDocument21 pagesTest Bank For Electronic Health Records and Nursing 1st Edition Richard Garteerosabellatrinh6a8o3No ratings yet
- 2015 Edition Proposed RuleDocument59 pages2015 Edition Proposed RuleVaibhav RaiNo ratings yet
- EHAQ 4th Cycle Audit Tool Final Feb.10-2022Document51 pagesEHAQ 4th Cycle Audit Tool Final Feb.10-2022Michael Gebreamlak100% (1)
- EU CER WhitepaperDocument5 pagesEU CER Whitepaperibrahim kademogluNo ratings yet
- Reqirement Specification Document FOR Hospital Management SystemDocument8 pagesReqirement Specification Document FOR Hospital Management Systemlekha soniNo ratings yet
- Tyagi SrsDocument21 pagesTyagi SrsMuskan SharmaNo ratings yet
- A Practical Guide To Meaningful Use: Federal Register, 75 (144), Wednesday, July 28, 2010, Pp. 44589-44654Document6 pagesA Practical Guide To Meaningful Use: Federal Register, 75 (144), Wednesday, July 28, 2010, Pp. 44589-44654dnice408No ratings yet
- Information ManagementDocument4 pagesInformation ManagementRegina TanioNo ratings yet
- Executive Summary: Software Requirements SpecificationDocument11 pagesExecutive Summary: Software Requirements SpecificationabhijeetpareekNo ratings yet
- Generalcertexchangeguidance Final 9-9-13Document5 pagesGeneralcertexchangeguidance Final 9-9-13Rashard Dyess-LaneNo ratings yet
- Eval MGMT Serv Guide ICN006764 PDFDocument90 pagesEval MGMT Serv Guide ICN006764 PDFPaula ChorazyNo ratings yet
- Software Requirements Specification For Patient Health Management SystemDocument8 pagesSoftware Requirements Specification For Patient Health Management Systemdilshad aliNo ratings yet
- 3rd Edition NABH Guidebook 2012 New PDFDocument258 pages3rd Edition NABH Guidebook 2012 New PDFraamki_99No ratings yet
- Practice Management IntergrationDocument5 pagesPractice Management Intergrationthe mad king readerNo ratings yet
- Project Report - Outdoor Patient Doctor's Booking SystemDocument51 pagesProject Report - Outdoor Patient Doctor's Booking SystemSoumya Kanti Ghosh100% (1)
- 2007 National Patient Safety Goals: For Those Programs Required To Complete A PPRDocument11 pages2007 National Patient Safety Goals: For Those Programs Required To Complete A PPRKenny JosefNo ratings yet
- Policy & Procure - HandoutDocument14 pagesPolicy & Procure - HandoutLaeeq R MalikNo ratings yet
- 4understanding The Breakdown of The Cost Report and The TFC RoleDocument16 pages4understanding The Breakdown of The Cost Report and The TFC RoleBalajiMGandhileNo ratings yet
- Asean MDPWG CSDT - Final - 21 Oct 2010Document12 pagesAsean MDPWG CSDT - Final - 21 Oct 2010Brian WilliamsNo ratings yet
- Software Requirement Specification Document For Hospital Management SystemDocument17 pagesSoftware Requirement Specification Document For Hospital Management Systemmegha_sinha_10100% (1)
- Executive Summary: Software Requirements Specification Revision HistoryDocument9 pagesExecutive Summary: Software Requirements Specification Revision HistorySwathi GattuNo ratings yet
- Class 4 - Electronic Health Record Systems - IshamaliDocument31 pagesClass 4 - Electronic Health Record Systems - IshamaliHanan AlkorashyNo ratings yet
- EHR and Meaningful UseDocument4 pagesEHR and Meaningful UseNkeletseng MakakaNo ratings yet
- Optum: A Health Services and Innovation CompanyDocument2 pagesOptum: A Health Services and Innovation CompanySui NarcanNo ratings yet
- Through: Dr. Alma B. Ungab, BSN, RN, MN, DPA Chief Nurse Vicente Sotto Memorial Medical Center B. Rodriguez ST., Cebu City, Philippines 6000Document1 pageThrough: Dr. Alma B. Ungab, BSN, RN, MN, DPA Chief Nurse Vicente Sotto Memorial Medical Center B. Rodriguez ST., Cebu City, Philippines 6000Sui NarcanNo ratings yet
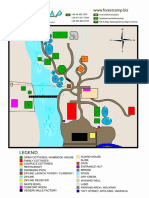
- Forest Camp Resort Map A4Document1 pageForest Camp Resort Map A4Sui NarcanNo ratings yet
- Optum Story 8.5x11 V1 PDFDocument2 pagesOptum Story 8.5x11 V1 PDFSui NarcanNo ratings yet
- Aspe Ceereal Breakfastbrochure FinalDocument16 pagesAspe Ceereal Breakfastbrochure FinalSui NarcanNo ratings yet
- Chronic Renal Failure To Esrd: Stage I Diminished Renal ReserveDocument3 pagesChronic Renal Failure To Esrd: Stage I Diminished Renal ReserveSui NarcanNo ratings yet
- Comprehensive Diagnostic Radiology Documentation: Prepared by The Zotec Corporate Coding DepartmentDocument43 pagesComprehensive Diagnostic Radiology Documentation: Prepared by The Zotec Corporate Coding DepartmentSui NarcanNo ratings yet
- Vital Signs Monitoring SheetDocument1 pageVital Signs Monitoring SheetSui NarcanNo ratings yet
- Resume EntrylevelDocument1 pageResume EntrylevelSui NarcanNo ratings yet
- You Can Heal Your LifeDocument173 pagesYou Can Heal Your LifeSui NarcanNo ratings yet
- ANA Code of Ethics For Nurses2Document6 pagesANA Code of Ethics For Nurses2Sui NarcanNo ratings yet
- Professional Entry Level ResumeDocument2 pagesProfessional Entry Level ResumeSui NarcanNo ratings yet
- Create Database VentasDocument11 pagesCreate Database VentasAnonymous BwTccxNo ratings yet
- UBC Athletics & Recreation: Purpose Requirement 3: Protect Stored Cardholder DataDocument2 pagesUBC Athletics & Recreation: Purpose Requirement 3: Protect Stored Cardholder DataMartha Jane LawheadNo ratings yet
- An Easy Look at The Cubic Formula: Osler@rowan - EduDocument7 pagesAn Easy Look at The Cubic Formula: Osler@rowan - EduSumit SehgalNo ratings yet
- Websphere Doctor 3 TdmaDocument16 pagesWebsphere Doctor 3 TdmaadnanbwNo ratings yet
- Does Analytics Trump IntuitionDocument2 pagesDoes Analytics Trump IntuitionSajeedNo ratings yet
- The Impact of Duplicate Medical Records and Overlays in HealthcareDocument15 pagesThe Impact of Duplicate Medical Records and Overlays in HealthcareJohn TraderNo ratings yet
- Techniques For Data Hiding-PDocument24 pagesTechniques For Data Hiding-PHarkirat ChawlaNo ratings yet
- A Review On Speech Recognition Challenges and ApproachesDocument7 pagesA Review On Speech Recognition Challenges and ApproachesWorld of Computer Science and Information Technology JournalNo ratings yet
- Seccionador - SchneiderDocument160 pagesSeccionador - SchneiderNicolás Santiago UgarteNo ratings yet
- Multilayer Perceptron: Architecture Optimization and TrainingDocument5 pagesMultilayer Perceptron: Architecture Optimization and TrainingaliceNo ratings yet
- Data Structure and Algorithum LAB 02Document8 pagesData Structure and Algorithum LAB 02earn moneyNo ratings yet
- CICS Aplication Programming Guide Dfhp3b00Document731 pagesCICS Aplication Programming Guide Dfhp3b00viriathvsNo ratings yet
- Nss Labs Sd-Wan Comparative ReportDocument9 pagesNss Labs Sd-Wan Comparative Reporteric1107No ratings yet
- Rahul@ResumeDocument2 pagesRahul@ResumeAakaram SaiprasadNo ratings yet
- Underscore Cheat SheetDocument1 pageUnderscore Cheat SheetasdfasldfhioNo ratings yet
- CPM Network Analysis FinalDocument33 pagesCPM Network Analysis Finalsonali kambleNo ratings yet
- CCS Powerpoint TemplateDocument18 pagesCCS Powerpoint TemplateJohn AudiNo ratings yet
- baitapTH CSDL KCNTT SVDocument5 pagesbaitapTH CSDL KCNTT SVSơn LongNo ratings yet
- Professional Practices VDocument4 pagesProfessional Practices VEr Amit GhadigaonkarNo ratings yet
- COD Model Descriere ProdusDocument6 pagesCOD Model Descriere ProdusMishu PavallNo ratings yet