You might also like
- 11 The Epidemiology of Intestinal MicrosporidiosisDocument7 pages11 The Epidemiology of Intestinal MicrosporidiosisDaniel VargasNo ratings yet
- The Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioDocument7 pagesThe Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioMaharaniNo ratings yet
- Effectiveness of Contact Isolation During A Hospital Outbreak of Methicillin-Resistant Staphylococcus AureusDocument9 pagesEffectiveness of Contact Isolation During A Hospital Outbreak of Methicillin-Resistant Staphylococcus Aureusmoniart2587No ratings yet
- Cryptosporidiosis in Children During A Massive Waterborne Outbreak in Milwaukee Wisconsin Clinical Laboratory and Epidemiologic FindingsDocument8 pagesCryptosporidiosis in Children During A Massive Waterborne Outbreak in Milwaukee Wisconsin Clinical Laboratory and Epidemiologic FindingsJOSE LUIS CARRASCO CHUQUILLANQUINo ratings yet
- Successful Treatment of Multiple Common Warts With Intralesional OzoneDocument6 pagesSuccessful Treatment of Multiple Common Warts With Intralesional OzoneRubensNo ratings yet
- A Hospital Based Prospective Study of Prevalence of Methicillin Resistant Staphylococcus Aureus in Dermatology Indoor Patients by Phenotypic MethodDocument9 pagesA Hospital Based Prospective Study of Prevalence of Methicillin Resistant Staphylococcus Aureus in Dermatology Indoor Patients by Phenotypic MethodIJAR JOURNALNo ratings yet
- A Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated with SurvivalDocument8 pagesA Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated with SurvivalAbrahamKatimeNo ratings yet
- Nebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaDocument4 pagesNebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaPhan Tấn TàiNo ratings yet
- Prevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityDocument11 pagesPrevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityAna LemesNo ratings yet
- The Emergence and Persistence of C Auris in Western New YorkDocument4 pagesThe Emergence and Persistence of C Auris in Western New YorkLilia JouNo ratings yet
- Kumar 2006Document8 pagesKumar 2006aiturraldeNo ratings yet
- 1 s2.0 S0002934322007227 MainDocument8 pages1 s2.0 S0002934322007227 MainMaryatiNo ratings yet
- Antibiotico YPronosticoDocument6 pagesAntibiotico YPronosticoagonzale52No ratings yet
- Epidemiology and Clinical Manifestations of Mucormycosis CMIDocument9 pagesEpidemiology and Clinical Manifestations of Mucormycosis CMIDINESH VENKATESANNo ratings yet
- 1 s2.0 S088539240300040X MainDocument6 pages1 s2.0 S088539240300040X MainPaula RNo ratings yet
- Highly Effective Against EsblDocument9 pagesHighly Effective Against Esblgaurav rawalNo ratings yet
- Hospital Acquired Infection Incidence and Risk FactorsDocument7 pagesHospital Acquired Infection Incidence and Risk FactorsKshitiz112No ratings yet
- Jurnal Interna 123456Document9 pagesJurnal Interna 123456vonnyandira28No ratings yet
- Ciz 1197Document8 pagesCiz 1197Lindia PrabhaswariNo ratings yet
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 pagesEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument11 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiNo ratings yet
- Utility of qSOFA and Modified SOFA in Severe Malaria Presenting As SepsisDocument13 pagesUtility of qSOFA and Modified SOFA in Severe Malaria Presenting As SepsisAhmad Zaki YamaniNo ratings yet
- Ebn RespiDocument17 pagesEbn RespilablabkurmNo ratings yet
- Antibiotics 11 01033 v4Document14 pagesAntibiotics 11 01033 v4Hana AoiNo ratings yet
- 3 Saritanayak EtalDocument7 pages3 Saritanayak EtaleditorijmrhsNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleTauhannyNo ratings yet
- Epidemiology RoundDocument13 pagesEpidemiology RoundFebniNo ratings yet
- IDSA Nec FascDocument34 pagesIDSA Nec FascShameen KhanNo ratings yet
- Golden Hour CCM Arthur Van Zanten IC1Document3 pagesGolden Hour CCM Arthur Van Zanten IC1Sara NicholsNo ratings yet
- Vivian I 2010Document11 pagesVivian I 2010Sumana MahankaliNo ratings yet
- Culture Negative SepsisDocument5 pagesCulture Negative SepsismalvindersahiNo ratings yet
- Literature Review of Plasmodium FalciparumDocument6 pagesLiterature Review of Plasmodium Falciparumea83xjp7100% (1)
- Fped 11 1303040Document8 pagesFped 11 1303040nadela noviaNo ratings yet
- Highly Active Antiretroviral Therapy and Viral ResDocument10 pagesHighly Active Antiretroviral Therapy and Viral ResIbrahim WahiedNo ratings yet
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDocument5 pagesAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanNo ratings yet
- IDSA Guidelines for Diagnosis and Management of Skin and Soft-Tissue InfectionsDocument34 pagesIDSA Guidelines for Diagnosis and Management of Skin and Soft-Tissue InfectionsROSEN NNo ratings yet
- Sphingomonas KoreensisDocument11 pagesSphingomonas KoreensisSMIBA MedicinaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Bacteriological Profile of Blood Stream Infections at A Rural Tertiary Care Teaching Hospital of Western Uttar PradeshDocument9 pagesBacteriological Profile of Blood Stream Infections at A Rural Tertiary Care Teaching Hospital of Western Uttar PradeshHArdik NegiNo ratings yet
- Antibiotic Enteric FeverDocument16 pagesAntibiotic Enteric FeverAnnisa SetyantiNo ratings yet
- The Frequency of Influenza and Bacterial Co-Infection - A SystematDocument12 pagesThe Frequency of Influenza and Bacterial Co-Infection - A Systematrahma_husna_1No ratings yet
- Difficile Infection and Colonization: Host and Pathogen Factors For ClostridiumDocument11 pagesDifficile Infection and Colonization: Host and Pathogen Factors For ClostridiumArif Rahman HakimNo ratings yet
- CandaDocument21 pagesCandazurique32No ratings yet
- Antibiotecoterapia en SepsisDocument13 pagesAntibiotecoterapia en SepsisJuan Pablo Arteaga VargasNo ratings yet
- Lee 2016Document8 pagesLee 2016Ali AbidNo ratings yet
- Russian FederationDocument5 pagesRussian FederationIngrid BenigayNo ratings yet
- MaybeDocument4 pagesMaybepertama bestNo ratings yet
- Epidemiology Roun1Document10 pagesEpidemiology Roun1FebniNo ratings yet
- Risk Factors and The Resistance Mechanisms Involved in Pseudomonas Aeruginosa Mutation in Critically Ill PatientsDocument9 pagesRisk Factors and The Resistance Mechanisms Involved in Pseudomonas Aeruginosa Mutation in Critically Ill PatientsElsiana LaurenciaNo ratings yet
- Adults Hospitalized With Pneumonia in The United States, Incidence, Epidemiologi, Mortality, 2017Document7 pagesAdults Hospitalized With Pneumonia in The United States, Incidence, Epidemiologi, Mortality, 2017Debi SusantiNo ratings yet
- Fungal Sepsis: Optimizing Antifungal Therapy in The Critical Care SettingDocument25 pagesFungal Sepsis: Optimizing Antifungal Therapy in The Critical Care SettingVineet GuptaNo ratings yet
- 8.A Case Report of Rabies With Long Incubation ImporDocument3 pages8.A Case Report of Rabies With Long Incubation ImporAndra CristianaNo ratings yet
- Jiaa 221Document13 pagesJiaa 221AndradaLavricNo ratings yet
- Providencia StuartiiDocument7 pagesProvidencia StuartiiNoviaCandraDwipaNo ratings yet
- Practice Guidelines For The Diagnosis and Management of Skin and Soft-Tissue InfectionsDocument34 pagesPractice Guidelines For The Diagnosis and Management of Skin and Soft-Tissue InfectionsNatalia MoranNo ratings yet
- DtifoDocument11 pagesDtifoDwi atikaNo ratings yet
- Isoniazid TuberculosisDocument10 pagesIsoniazid TuberculosisAisyah Aftita KamrasyidNo ratings yet
- Parasitic Infections and the Immune SystemFrom EverandParasitic Infections and the Immune SystemFelipe KierzenbaumNo ratings yet
- Glossary of Anatomical TermsDocument69 pagesGlossary of Anatomical TermsJohnNo ratings yet
- Clinical Relevance of Mupirocin Resistance in Staphylococcus Aureus - Elsevier Enhanced ReaderDocument9 pagesClinical Relevance of Mupirocin Resistance in Staphylococcus Aureus - Elsevier Enhanced ReaderJohnNo ratings yet
- Mupirocin ResistanceDocument7 pagesMupirocin ResistanceJohnNo ratings yet
- A Review On Mechanism of Action, Resistance, Synergism, and Clinical Implications of Mupirocin Against Staphylococcus Aureus - Elsevier Enhanced ReaderDocument11 pagesA Review On Mechanism of Action, Resistance, Synergism, and Clinical Implications of Mupirocin Against Staphylococcus Aureus - Elsevier Enhanced ReaderJohnNo ratings yet
- Treatment of Staphylococcus Aureus Colonization and Prophylaxis For Infection With Topical Intranasal Mupirocin: An Evidence-Based ReviewDocument6 pagesTreatment of Staphylococcus Aureus Colonization and Prophylaxis For Infection With Topical Intranasal Mupirocin: An Evidence-Based ReviewJohnNo ratings yet
- Plaza of The Americas: Please NoteDocument1 pagePlaza of The Americas: Please NoteJohnNo ratings yet
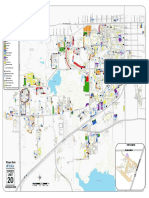
- 2013 Parking MapDocument1 page2013 Parking MapJohnNo ratings yet
- Rider's Guide To Real CollectionDocument1 pageRider's Guide To Real CollectionNikkiKirkNo ratings yet
- Periodic Table: ChemistryDocument1 pagePeriodic Table: ChemistryRafael RamosNo ratings yet
- Climate RefugeesDocument9 pagesClimate RefugeesJohnNo ratings yet
- Siddhartha and Van GoghDocument3 pagesSiddhartha and Van GoghJohnNo ratings yet
- Aplastic Anemia Is A NormocyticDocument17 pagesAplastic Anemia Is A NormocyticAfrio ArismanNo ratings yet
- Intestinal Surgery in Small Animals - How To Prevent It Leaking?Document5 pagesIntestinal Surgery in Small Animals - How To Prevent It Leaking?Ayu DinaNo ratings yet
- 678 FullDocument9 pages678 FullDarren WilliamNo ratings yet
- Typhoid DiseaseDocument28 pagesTyphoid DiseaseSaba Parvin Haque100% (1)
- Nutrition During Pregnancy and LactationDocument240 pagesNutrition During Pregnancy and LactationDede MashaNo ratings yet
- Ribeiro Et Al. - 2018 - Journal of The American College of Nutrition Influence of The C677T Polymorphism of The MTHFR Gene On OxidativeDocument9 pagesRibeiro Et Al. - 2018 - Journal of The American College of Nutrition Influence of The C677T Polymorphism of The MTHFR Gene On OxidativerafaellapordeusNo ratings yet
- Brand Plan for Metformin XRDocument47 pagesBrand Plan for Metformin XRSanket UmredkarNo ratings yet
- Functions of the Digestive System ExplainedDocument32 pagesFunctions of the Digestive System ExplainedAubrey Cissé MwakayeNo ratings yet
- Edema in Renal DiseaseDocument3 pagesEdema in Renal DiseasePathrecia Natalia SiagianNo ratings yet
- MCQ Final 1910Document20 pagesMCQ Final 1910JohnSonNo ratings yet
- 2nd Mental Health Forum (With Background)Document4 pages2nd Mental Health Forum (With Background)Aj CamachoNo ratings yet
- DAST-10 Institute PDFDocument1 pageDAST-10 Institute PDFImran KhanNo ratings yet
- Lecture 8 Notes AggressionDocument6 pagesLecture 8 Notes AggressionCeline SinghNo ratings yet
- Bioprotexion Manual Virocid VirocidDocument9 pagesBioprotexion Manual Virocid Virocidabd el rhman gamalNo ratings yet
- Liu 2017-Herbal Medicine For The Treatment of ObesityDocument17 pagesLiu 2017-Herbal Medicine For The Treatment of ObesityMas NuriNo ratings yet
- Cisplatin Versus Carboplatin For Patients With Metastatic Non - Small-Cell Lung Cancer - An Old Rivalry RenewedDocument2 pagesCisplatin Versus Carboplatin For Patients With Metastatic Non - Small-Cell Lung Cancer - An Old Rivalry RenewedFlorin RizicaNo ratings yet
- FAMILY NURSING CARE PLAN - Presence of Breeding Sites For Insects and PestsDocument2 pagesFAMILY NURSING CARE PLAN - Presence of Breeding Sites For Insects and PestsJULIANNE BAYHON100% (1)
- Factors Responsible for Foodborne DiseasesDocument3 pagesFactors Responsible for Foodborne DiseasesSayp dNo ratings yet
- Cliques in Cms High Schools and The Consequences Final PaperDocument8 pagesCliques in Cms High Schools and The Consequences Final Paperapi-441877801No ratings yet
- Features Interview exposes hidden "noiseDocument5 pagesFeatures Interview exposes hidden "noiseMy SơnNo ratings yet
- Managing Health and Safety in HealthcareDocument56 pagesManaging Health and Safety in HealthcareKamlesh KumarNo ratings yet
- Final Draft Sheraz Akbar FA18-BPY-084Document162 pagesFinal Draft Sheraz Akbar FA18-BPY-084Ali AmadNo ratings yet
- Hemodialysis TrainingDocument2 pagesHemodialysis TrainingHarby80% (5)
- 10 Effect of UV Light and Temperature On Bacterial GrowthDocument4 pages10 Effect of UV Light and Temperature On Bacterial GrowthMaui Vecinal de GuzmanNo ratings yet
- Nursing Care Plan-Epigastric PainDocument2 pagesNursing Care Plan-Epigastric PainK-anne Cherubic100% (3)
- Nur - 100 Session 2 - SemillaDocument6 pagesNur - 100 Session 2 - SemillaVon R Semilla100% (1)
- Neural Differentiation of Human Pluripotent Stem CellsDocument12 pagesNeural Differentiation of Human Pluripotent Stem Cellsilmiah neurologiNo ratings yet
- Fellowship in Critical Care MedicineDocument12 pagesFellowship in Critical Care MedicinerajiNo ratings yet
- The Germ Theory of Disease and Philippine Revolutionary ScientistsDocument15 pagesThe Germ Theory of Disease and Philippine Revolutionary ScientistsAmi MizunoNo ratings yet
- Efektifitas Pemberian Wedang Jahe terhadap Frekuensi Mual dan Muntah pada Ibu Hamil Trimester IDocument11 pagesEfektifitas Pemberian Wedang Jahe terhadap Frekuensi Mual dan Muntah pada Ibu Hamil Trimester IrohyatiNo ratings yet