You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Quality and Patient Safety ChecklistDocument7 pagesQuality and Patient Safety ChecklistKarl Roble100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Automatic Medicine Vending Machine: Problem StatementDocument8 pagesAutomatic Medicine Vending Machine: Problem StatementRudresh RakeshNo ratings yet
- AAMI FDA Summit Report PDFDocument48 pagesAAMI FDA Summit Report PDFNoe Muñoz QuitoNo ratings yet
- ACS StandardsDocument63 pagesACS StandardsColleen CalditoNo ratings yet
- 10 Simulation Exercises As A Patient Safety Strategy PDFDocument9 pages10 Simulation Exercises As A Patient Safety Strategy PDFAmanda DavisNo ratings yet
- Soal Bahasa Inggris 2aDocument19 pagesSoal Bahasa Inggris 2aMegaaNo ratings yet
- J C. W, CHC, PMP, CMGV C M G S: Changes in The Medical Gas and Vacuum System RequirementsDocument119 pagesJ C. W, CHC, PMP, CMGV C M G S: Changes in The Medical Gas and Vacuum System RequirementsCarmenDominguezJaraNo ratings yet
- Analisis Faktor Pendukung Dan Penghambat Budaya Keselamatan Pasien Di Rumah SakitDocument7 pagesAnalisis Faktor Pendukung Dan Penghambat Budaya Keselamatan Pasien Di Rumah SakitAyueNo ratings yet
- Clinical Practice Guideline Safe Medication Use.32Document39 pagesClinical Practice Guideline Safe Medication Use.32Edward ZiyachechaNo ratings yet
- Sentinel Event PaperDocument18 pagesSentinel Event PaperChelsea RuthrauffNo ratings yet
- Communication Skills Education For Doctors: An UpdateDocument50 pagesCommunication Skills Education For Doctors: An UpdateDaniel PendickNo ratings yet
- Tni PaperDocument7 pagesTni Paperapi-298609879No ratings yet
- Principles of Patient'S Safety: Basic Health Skills (GRU1251)Document39 pagesPrinciples of Patient'S Safety: Basic Health Skills (GRU1251)attooNo ratings yet
- GLP Part 1 Subpart ADocument4 pagesGLP Part 1 Subpart AGURPREET SINGHNo ratings yet
- 10 Documented Operational and Maintenance (Preventive and Breakdown) Plan For Clinical and Support Service EquipmentDocument38 pages10 Documented Operational and Maintenance (Preventive and Breakdown) Plan For Clinical and Support Service EquipmentSanjay Kadam100% (1)
- What Exactly Is Patient SafetyDocument19 pagesWhat Exactly Is Patient Safetybe a doctor for you Medical studentNo ratings yet
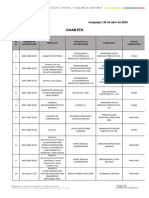
- Guantes: ITE M Número de Autorización Producto Titular de La Autorización Fabricante País de FabricaciónDocument2 pagesGuantes: ITE M Número de Autorización Producto Titular de La Autorización Fabricante País de FabricaciónAdrian AstorgaNo ratings yet
- An Investigation and Assessment Study: A Basis For The Proposed Development of Rogaciano M. Mercado Memorial HospitalDocument55 pagesAn Investigation and Assessment Study: A Basis For The Proposed Development of Rogaciano M. Mercado Memorial HospitalMark Ryan NagalesNo ratings yet
- Full Chapter Complete Revision Guide For Mrcog Part 3 1St Edition Justin C Konje PDFDocument53 pagesFull Chapter Complete Revision Guide For Mrcog Part 3 1St Edition Justin C Konje PDFsteven.owens745100% (2)
- Resume 2010Document2 pagesResume 2010Paul ArmstrongNo ratings yet
- Pengaruh Pendidikan Kesehatan Metode Demonstrasi Terhadap Hand Hygiene 6 Langkah 5 Momen Keluarga PasienDocument10 pagesPengaruh Pendidikan Kesehatan Metode Demonstrasi Terhadap Hand Hygiene 6 Langkah 5 Momen Keluarga PasienRiA NDARINo ratings yet
- RFID Past DecadeDocument4 pagesRFID Past DecadeReadstoryNo ratings yet
- Evidence-Based Practice: QSEN, 2015Document3 pagesEvidence-Based Practice: QSEN, 2015Edwin MwangiNo ratings yet
- PSQCM ProjectDocument9 pagesPSQCM Projectapi-371817203No ratings yet
- MATERI PAK KuncoroDocument27 pagesMATERI PAK KuncoroanjariNo ratings yet
- Clinical ReasoningDocument4 pagesClinical Reasoningapi-351971578No ratings yet
- Wards Nursing ServicesDocument17 pagesWards Nursing ServicesMohammed HamedNo ratings yet
- Patient Transfer Policy 3.0Document25 pagesPatient Transfer Policy 3.0Val SolidumNo ratings yet
- Patient Safety Executive Summary 10052014Document11 pagesPatient Safety Executive Summary 10052014aridloNo ratings yet
- Nursing Care Framework - Version 1Document22 pagesNursing Care Framework - Version 1chelissa maitaNo ratings yet