You might also like
- Isolation TechniqueDocument19 pagesIsolation Techniquejenn21283% (6)
- The Infection Control Manual: Standard PrecautionsDocument5 pagesThe Infection Control Manual: Standard Precautionszenagit123456No ratings yet
- SOP 2: Outdoor Patient Management: 1. PurposeDocument11 pagesSOP 2: Outdoor Patient Management: 1. Purposeshah007zaad100% (1)
- Facility Management SystemDocument6 pagesFacility Management Systemshah007zaad100% (1)
- Isolated Inpatient Ward of 50 Beds: Plan, Staff Organise and Develop AnDocument8 pagesIsolated Inpatient Ward of 50 Beds: Plan, Staff Organise and Develop AnakinravNo ratings yet
- Protocol For Infection Control and Isolation ward-COVID-19Document17 pagesProtocol For Infection Control and Isolation ward-COVID-19RQAU SALEM QUALITY ASSURANCE PROGRAMNo ratings yet
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFAmjadali ChoudhariNo ratings yet
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFSaurav KumarNo ratings yet
- Office of The Secretary: AreasDocument9 pagesOffice of The Secretary: AreasJoshua Espanto MorenNo ratings yet
- HostDocument21 pagesHostJoanna DagohoyNo ratings yet
- Personal Protective Equipment (PPE) - Equipment That Creates A Barrier Between InfectiousDocument4 pagesPersonal Protective Equipment (PPE) - Equipment That Creates A Barrier Between InfectiousJp Rizal IPCCNo ratings yet
- Barrier NursingDocument5 pagesBarrier NursingShiny Preethi100% (1)
- Issues Related To Kidney Disease and HypertensionDocument12 pagesIssues Related To Kidney Disease and HypertensionCarlos Huaman ZevallosNo ratings yet
- Revised Guidelines For Home Isolation of Mild and Asymptomatic COVID-19 CasesDocument7 pagesRevised Guidelines For Home Isolation of Mild and Asymptomatic COVID-19 CasesNDTV100% (11)
- Standard Operating ProcedureDocument15 pagesStandard Operating ProcedureAyman AliNo ratings yet
- Universal PrecautionsDocument4 pagesUniversal PrecautionsRasheena Alaja JainalNo ratings yet
- 3 PDFDocument59 pages3 PDFnaveen kumarNo ratings yet
- Isolation Precautions: Personal Protective Equipment: Extended TextDocument13 pagesIsolation Precautions: Personal Protective Equipment: Extended TextIonut ChicinasNo ratings yet
- Isolation Precautions: Airborne - CE: AlertDocument11 pagesIsolation Precautions: Airborne - CE: AlertNama ManaNo ratings yet
- 3364 109 Iso 404Document7 pages3364 109 Iso 404mediaaprinaNo ratings yet
- Group 3 - NCM 119 Case Scenario - Bartolata-4ADocument6 pagesGroup 3 - NCM 119 Case Scenario - Bartolata-4AKeisha BartolataNo ratings yet
- Prepration of The Isolation UnitDocument43 pagesPrepration of The Isolation UnitGayatri MudliyarNo ratings yet
- Home Isolation GuidelinesDocument17 pagesHome Isolation GuidelinesDigambar S TatkareNo ratings yet
- Annex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Document4 pagesAnnex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Yeoh Zi-NingNo ratings yet
- Topic B Topic Title: Surgical and Medical Asepsis Topic ObjectivesDocument16 pagesTopic B Topic Title: Surgical and Medical Asepsis Topic ObjectivesZyrene RiveraNo ratings yet
- Isolation PrecautionsDocument13 pagesIsolation Precautionsmalyn1218No ratings yet
- ASepsisDocument52 pagesASepsisnew biee100% (1)
- Standard Precautions: 1.1 Hand HygieneDocument9 pagesStandard Precautions: 1.1 Hand HygieneSandra Ann BijuNo ratings yet
- Test 1: The Incubation Period For Chickenpox Is Usually 14 To 16 Days But Can Range From 10 To 21 DaysDocument4 pagesTest 1: The Incubation Period For Chickenpox Is Usually 14 To 16 Days But Can Range From 10 To 21 DaysLillabinNo ratings yet
- Infection Control and Prevention Protocols in Hotel Housekeeping (Final)Document44 pagesInfection Control and Prevention Protocols in Hotel Housekeeping (Final)Celso Jr FelipeNo ratings yet
- Isolation PrecautionsDocument58 pagesIsolation PrecautionsDrShereen Fawzy HafezNo ratings yet
- Kis and MegDocument31 pagesKis and MegkisNo ratings yet
- Monkeypox ProtocolDocument10 pagesMonkeypox ProtocolrhferanielNo ratings yet
- Universal Precautions (UP)Document26 pagesUniversal Precautions (UP)Avigael Gabriel AvilesNo ratings yet
- National Guidelines For Safe Dental Practice During Covid-19 PandemicDocument7 pagesNational Guidelines For Safe Dental Practice During Covid-19 PandemicSatisha TSNo ratings yet
- Hap Lo5Document8 pagesHap Lo5cjNo ratings yet
- Infection ControlDocument16 pagesInfection ControlMohamed AbdelkaderNo ratings yet
- Australia Covid PpeDocument5 pagesAustralia Covid PpeAbidi HichemNo ratings yet
- MOB MECQ GuidelinesDocument18 pagesMOB MECQ GuidelinesTeng GanzonNo ratings yet
- WHO EVD Guidance IPC 14.1 EngDocument6 pagesWHO EVD Guidance IPC 14.1 Engdhoo_babyNo ratings yet
- COVID-19 Preparedness 14apr2020Document13 pagesCOVID-19 Preparedness 14apr2020Andre3893No ratings yet
- Sec 1 1 STD Trans Precautions-2019-01 - FINALDocument19 pagesSec 1 1 STD Trans Precautions-2019-01 - FINALElaine UrgeNo ratings yet
- UHMS Guidelines - COVID-19 V4Document3 pagesUHMS Guidelines - COVID-19 V4Juan CruzNo ratings yet
- Harmonized TTMF Assessment-Tool Final Draft Jul 27 2020Document10 pagesHarmonized TTMF Assessment-Tool Final Draft Jul 27 2020Jay EspinalNo ratings yet
- Guidelines For Safe ENT Practice in COVID 19Document12 pagesGuidelines For Safe ENT Practice in COVID 19muzeebur rahmanNo ratings yet
- Entcovid0306 PDFDocument12 pagesEntcovid0306 PDFPriyanka KolluruNo ratings yet
- IPC in HD ServicesDocument28 pagesIPC in HD ServicesseptianyganescyaNo ratings yet
- MdroDocument14 pagesMdroreynoldNo ratings yet
- Draft Letter For Reusable PPE Version 2Document5 pagesDraft Letter For Reusable PPE Version 2Arlene AngelesNo ratings yet
- 2 Infection Prevention and ControlDocument5 pages2 Infection Prevention and ControlLiane BartolomeNo ratings yet
- Suraj Clinical Management of COVID 19Document23 pagesSuraj Clinical Management of COVID 19H.M RathodNo ratings yet
- EC-06-001 - Standard and Transmission Based PrecautionsDocument24 pagesEC-06-001 - Standard and Transmission Based PrecautionsBezawit YosefNo ratings yet
- Infection Control Manual: Policy Name Policy Number Date This Version Effective Responsible For ContentDocument5 pagesInfection Control Manual: Policy Name Policy Number Date This Version Effective Responsible For Contentحثيث علي يحيى مطهر100% (1)
- Standard PrecautionsDocument4 pagesStandard PrecautionsEthel May AlabastroNo ratings yet
- Guidelines On Preventive Measures To Contain Spread of COVID-19 in WorkplaceDocument10 pagesGuidelines On Preventive Measures To Contain Spread of COVID-19 in WorkplaceGEET SAWHNEYNo ratings yet
- IPC GUIDELINE Version 2Document20 pagesIPC GUIDELINE Version 2Nrs KhalidNo ratings yet
- 03.12 - Environmental and Equipment Cleaning and Disinfection in Rooms With Patients With An Emerging Infectious Disease (EID)Document10 pages03.12 - Environmental and Equipment Cleaning and Disinfection in Rooms With Patients With An Emerging Infectious Disease (EID)Adzkiya Az ZahraNo ratings yet
- Clinical Ward CatedralDocument4 pagesClinical Ward Catedralje-ann catedralNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesFrom EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesNo ratings yet
- Basic Guide to Infection Prevention and Control in DentistryFrom EverandBasic Guide to Infection Prevention and Control in DentistryNo ratings yet
- Policy On Narcotic and Psychotropic DrugsDocument10 pagesPolicy On Narcotic and Psychotropic Drugsshah007zaadNo ratings yet
- SOP 8, 20: OT and CSSD: 1. PurposeDocument9 pagesSOP 8, 20: OT and CSSD: 1. Purposeshah007zaadNo ratings yet
- Radiology ServicesDocument5 pagesRadiology Servicesshah007zaadNo ratings yet
- Inventory and StoreDocument4 pagesInventory and Storeshah007zaadNo ratings yet
- Accident and Emergency DepartmentDocument9 pagesAccident and Emergency Departmentshah007zaadNo ratings yet
- Inpatient DepartmentDocument7 pagesInpatient Departmentshah007zaadNo ratings yet
- Hospital Disaster PlanDocument91 pagesHospital Disaster Planshah007zaad100% (3)
- Sop Icu H & FW 12725 28.04.2018Document20 pagesSop Icu H & FW 12725 28.04.2018shah007zaadNo ratings yet
- Guidelines On Clinical Management of Covid - 19Document15 pagesGuidelines On Clinical Management of Covid - 19shah007zaadNo ratings yet
- Legal Liabilities of DoctorDocument4 pagesLegal Liabilities of Doctorshah007zaadNo ratings yet
- Dose ResponseDocument42 pagesDose ResponseHend maarofNo ratings yet
- Vinmec InvoiceDocument7 pagesVinmec InvoiceLyon HuynhNo ratings yet
- Mefenamic AcidDocument3 pagesMefenamic AcidAngelica Cassandra VillenaNo ratings yet
- N PDFDocument136 pagesN PDFDr-Jahanzaib GondalNo ratings yet
- MycotoxinsDocument4 pagesMycotoxinsnepoliyan ghimireNo ratings yet
- Radiologic Pathology Intro 1Document50 pagesRadiologic Pathology Intro 1James MoralesNo ratings yet
- PubMedHealth PMH0091057Document377 pagesPubMedHealth PMH0091057Jose ManuelNo ratings yet
- PHQ-9 GoodDocument9 pagesPHQ-9 GoodJorge GámezNo ratings yet
- OsteosarcomaDocument24 pagesOsteosarcomaBakta GiriNo ratings yet
- Cook County Jail COVID-19 Federal LawsuitDocument30 pagesCook County Jail COVID-19 Federal LawsuitAdam HarringtonNo ratings yet
- 2000 Nclex MS Sample QuestionDocument314 pages2000 Nclex MS Sample QuestionElizabella Henrietta TanaquilNo ratings yet
- Beaconhouse School System: Latifabad Secondary Branch Marking Key Assessment 2015 SCIENCE - VIIIDocument1 pageBeaconhouse School System: Latifabad Secondary Branch Marking Key Assessment 2015 SCIENCE - VIIIBio & Chemistry LoversNo ratings yet
- Reflection PaperDocument3 pagesReflection PaperBRENCY CLAIRE ALURANNo ratings yet
- Memory Loss PDFDocument11 pagesMemory Loss PDFAbbas KhanNo ratings yet
- Mrs. Manisha Chichani 29032023 064453 PMDocument1 pageMrs. Manisha Chichani 29032023 064453 PMManisha ChichaniNo ratings yet
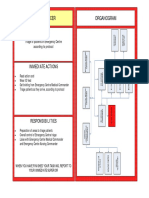
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- Scally - Anabolic Steroids - A Question of MuscleDocument0 pagesScally - Anabolic Steroids - A Question of MuscleFabian MolinaNo ratings yet
- Book PDFDocument186 pagesBook PDFLuis CcenchoNo ratings yet
- Universal Principles of NCMDocument43 pagesUniversal Principles of NCM+nella100% (1)
- Ucmi Newsletter July/august 2023Document3 pagesUcmi Newsletter July/august 2023UCMISTPNo ratings yet
- Science9 - q1 - Module1 - Respiratoryandcirculatorysystemsworkingtogether v2.0Document26 pagesScience9 - q1 - Module1 - Respiratoryandcirculatorysystemsworkingtogether v2.0Twela Dea Dela CruzNo ratings yet
- Anti-Candidal Activity and Synergetic Interaction of Antifungal Drugs WithDocument11 pagesAnti-Candidal Activity and Synergetic Interaction of Antifungal Drugs WithsivarajNo ratings yet
- Chapter 5: Treatment For Latent Tuberculosis InfectionDocument30 pagesChapter 5: Treatment For Latent Tuberculosis InfectionPhilippe Ceasar C. BascoNo ratings yet
- Georgia Living WillDocument9 pagesGeorgia Living WillRocketLawyer100% (2)
- Article 1509431938Document3 pagesArticle 1509431938AnujNo ratings yet
- Solitary Fibrous Tumor of Parotid Gland 2022Document6 pagesSolitary Fibrous Tumor of Parotid Gland 2022Reyes Ivan García CuevasNo ratings yet
- Compare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenDocument12 pagesCompare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenAamir BugtiNo ratings yet
- Assessing Eyes NCM 103 ChecklistDocument7 pagesAssessing Eyes NCM 103 ChecklistNicole NipasNo ratings yet
- Health DefecienciesDocument2 pagesHealth DefecienciesRainel Manos100% (1)
- Food Grade Hydrogen Peroxide - Suggested Uses and WarningsDocument1 pageFood Grade Hydrogen Peroxide - Suggested Uses and Warningsziba100% (1)