You might also like
- Drug Screening Test Info PDFDocument11 pagesDrug Screening Test Info PDFabid fahruddinNo ratings yet
- Non Medical Prescribing Using The British National Formulary PDFDocument6 pagesNon Medical Prescribing Using The British National Formulary PDFRyan MwNo ratings yet
- Oral Contraceptives PresentationDocument19 pagesOral Contraceptives PresentationJoshua DayeNo ratings yet
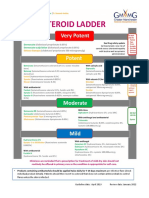
- GM Steroid LadderDocument2 pagesGM Steroid LadderRenee McGuinnessNo ratings yet
- Pharmacogenetics and The Concept of Individualized Medicine: BS ShastryDocument6 pagesPharmacogenetics and The Concept of Individualized Medicine: BS Shastrykunalprabhu148No ratings yet
- Pharmaceutical Aspects of Cancer Chemotherapy: Topics in PharmacyFrom EverandPharmaceutical Aspects of Cancer Chemotherapy: Topics in PharmacyA. T. FlorenceNo ratings yet
- Drug Index Updated2Document113 pagesDrug Index Updated2tam meiNo ratings yet
- Formulation Factors in Adverse Reactions: Topics in PharmacyFrom EverandFormulation Factors in Adverse Reactions: Topics in PharmacyA. T. FlorenceNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Assessment Report Cyproterone Acetate/ethinylestradiol (2 mg/0.035 MG) Containing Medicinal ProductsDocument39 pagesAssessment Report Cyproterone Acetate/ethinylestradiol (2 mg/0.035 MG) Containing Medicinal ProductsFinna ChatrineNo ratings yet
- Metamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical Profile PDFDocument16 pagesMetamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical Profile PDFcristirusu23No ratings yet
- Metamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical ProfileDocument16 pagesMetamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical ProfileTifanny WijayaNo ratings yet
- Drug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver DiseaseDocument20 pagesDrug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver Diseaseal ghiffari muhammad rayhan100% (1)
- Paracetamol Toxicity An Overview 2165 7548.1000158Document3 pagesParacetamol Toxicity An Overview 2165 7548.1000158psNo ratings yet
- 95 101 Hepatotoxicity of Paracetamol and Related FatalitiesDocument7 pages95 101 Hepatotoxicity of Paracetamol and Related Fatalitiesfabrizzio asdasdNo ratings yet
- Sulfamethoxazole Trimethoprim PDFDocument10 pagesSulfamethoxazole Trimethoprim PDFAsi SyyffaNo ratings yet
- 01156Document13 pages01156riskysetNo ratings yet
- Eso AmitriptilinDocument8 pagesEso AmitriptilinNurhasna Sushmita SariNo ratings yet
- Antiemetic Drug Class ReviewDocument24 pagesAntiemetic Drug Class ReviewNyume Lathifah HanumNo ratings yet
- WC 500003409Document12 pagesWC 500003409TowhidulIslamNo ratings yet
- Drug-Induced Hepatotoxicity: BackgroundDocument13 pagesDrug-Induced Hepatotoxicity: BackgroundrianiNo ratings yet
- Dyspepsia Templated UploadDocument5 pagesDyspepsia Templated UploadmasrafaumasugiNo ratings yet
- Antisense Therapy - WikipediaDocument17 pagesAntisense Therapy - Wikipediasattyadev95No ratings yet
- Nimesulide Patients Still Exposed To A Risk of Severe HepatitisDocument2 pagesNimesulide Patients Still Exposed To A Risk of Severe Hepatitisbrown_chocolate87643No ratings yet
- Journal Pone 0265305Document15 pagesJournal Pone 0265305Hanif Ibnu FauzyNo ratings yet
- Bahar Et Al-2017-Pharmacoepidemiology and Drug SafetyDocument14 pagesBahar Et Al-2017-Pharmacoepidemiology and Drug SafetyAdin RamadhanNo ratings yet
- Graduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainDocument3 pagesGraduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainaillNo ratings yet
- Bartzela-Maltha2016 Chapter MedicationEffectsOnTheRateOfOrDocument27 pagesBartzela-Maltha2016 Chapter MedicationEffectsOnTheRateOfOrcdmartinavalletteNo ratings yet
- 02 Pharmacological Drugs Inducing OtotoxicityDocument36 pages02 Pharmacological Drugs Inducing OtotoxicityKrisna PonggalungguNo ratings yet
- Immunosuppressive Drug TherapyDocument25 pagesImmunosuppressive Drug Therapyapi-3741769100% (2)
- Thionamides: Side Effects and ToxicitiesDocument11 pagesThionamides: Side Effects and ToxicitiesJesús MoraNo ratings yet
- Wu 2013Document4 pagesWu 2013Luisa Fernanda Rojas DiazNo ratings yet
- Farmacocinetica y Dinamia en Adultdos MayoresDocument5 pagesFarmacocinetica y Dinamia en Adultdos MayoresDIEGO FERNANDO URIBE JARAMILLONo ratings yet
- Paracetamol: Mechanism of Action, Applications and Safety ConcernDocument22 pagesParacetamol: Mechanism of Action, Applications and Safety ConcernIna SuciNo ratings yet
- Teratogenic Mechanisms of Medical DrugsDocument17 pagesTeratogenic Mechanisms of Medical DrugsKarol Valeria Garcia GonzalezNo ratings yet
- Risk Managment Plan TemplateDocument21 pagesRisk Managment Plan TemplatetovishwanathNo ratings yet
- s00404 019 05340 4Document8 pagess00404 019 05340 4Tanaporn ThongpolNo ratings yet
- MMF Rev Médica de Chile 2022Document8 pagesMMF Rev Médica de Chile 2022Martin RebellaNo ratings yet
- Pharmacological Interactions of VasoconstrictorsDocument8 pagesPharmacological Interactions of VasoconstrictorsValeska Farina EspinosaNo ratings yet
- 1471 2431 11 15Document9 pages1471 2431 11 15jessicacookNo ratings yet
- Romano 2018Document24 pagesRomano 2018Rizqan Fahlevvi AkbarNo ratings yet
- Medicines Available Pre-/post World War 2 Pre WW2 Post WW2Document4 pagesMedicines Available Pre-/post World War 2 Pre WW2 Post WW2ZNo ratings yet
- Ima 3Document7 pagesIma 3Nony KumalasariNo ratings yet
- Pediatric Non-Hodgkin Lymphoma MedicationDocument8 pagesPediatric Non-Hodgkin Lymphoma MedicationtopNo ratings yet
- Jardiance Epar Public Assessment Report - en PDFDocument99 pagesJardiance Epar Public Assessment Report - en PDFmanoj bhattaraiNo ratings yet
- Update On The Incidence of Metamizole Sodium-Induced Blood Dyscrasias in PolandDocument7 pagesUpdate On The Incidence of Metamizole Sodium-Induced Blood Dyscrasias in PolandNegreanu AncaNo ratings yet
- Update On The Incidence of Metamizole Sodium-Induced Blood Dyscrasias in PolandDocument7 pagesUpdate On The Incidence of Metamizole Sodium-Induced Blood Dyscrasias in PolandNegreanu AncaNo ratings yet
- Zhou2008 Vis DujDocument47 pagesZhou2008 Vis DujAnAn BanhGaoNo ratings yet
- Drug Interactions: The Clinician S Approach ToDocument11 pagesDrug Interactions: The Clinician S Approach ToGaby ValenzuelaNo ratings yet
- 2018 PharmacogeneticspaperDocument17 pages2018 PharmacogeneticspaperKatzumi MartinezNo ratings yet
- Trends in Tramadol: Pharmacology, Metabolism, and MisuseDocument11 pagesTrends in Tramadol: Pharmacology, Metabolism, and MisuseaksinuNo ratings yet
- Teratogenic Mechanisms of MedicalDocument17 pagesTeratogenic Mechanisms of MedicalLeandro V. L.No ratings yet
- T H e C U R B S I D e C o N S U L TDocument7 pagesT H e C U R B S I D e C o N S U L TwaftmoversNo ratings yet
- Mono Trypsin EnglishDocument5 pagesMono Trypsin EnglishTom DelongeNo ratings yet
- IntoxicationDocument7 pagesIntoxicationEmőke MátyásNo ratings yet
- Upper Gastrointestinal Bleeding Associated With Antiplatelet DrugsDocument8 pagesUpper Gastrointestinal Bleeding Associated With Antiplatelet DrugsAmalia NandiaNo ratings yet
- Pharmacogenetics of Cardiovascular Drug TherapyDocument11 pagesPharmacogenetics of Cardiovascular Drug Therapybalaji5563No ratings yet
- Pharmacology of MetforminDocument11 pagesPharmacology of MetforminkartikawensdiNo ratings yet
- Anticonvulsivantes Mecanismos de AccionDocument23 pagesAnticonvulsivantes Mecanismos de Accionmondragon_cortesNo ratings yet
- Metformin: Not Only Per Os: Expert Review of Endocrinology & MetabolismDocument6 pagesMetformin: Not Only Per Os: Expert Review of Endocrinology & MetabolismwachoNo ratings yet
- A Career in The Pharmaceutical SciencesDocument19 pagesA Career in The Pharmaceutical SciencesDrSandeep NarulaNo ratings yet
- Asthma ReviewDocument12 pagesAsthma ReviewMaria SalakoNo ratings yet
- Journal of International Medical Research 2010 Basak 1374 80Document7 pagesJournal of International Medical Research 2010 Basak 1374 80Zaidan FailasufaNo ratings yet
- Drug Study DiazepamDocument2 pagesDrug Study DiazepamBunnie AlphaNo ratings yet
- Daftar Harga Ethical Per April'22 (Khus Riau)Document8 pagesDaftar Harga Ethical Per April'22 (Khus Riau)iraNo ratings yet
- Drugs Acting On UterusDocument19 pagesDrugs Acting On Uterus101 102No ratings yet
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration Summarywilltippin4747No ratings yet
- BupropionDocument3 pagesBupropionRJ HNo ratings yet
- Heparin and Insulin DripsDocument11 pagesHeparin and Insulin DripsCeleste Chapman100% (2)
- CElegans NetworkDocument893 pagesCElegans NetworkMelissa HaganNo ratings yet
- 1pharma Lecture 1Document17 pages1pharma Lecture 1Mahnoor OmarNo ratings yet
- Rene ProductDocument8 pagesRene ProductBhakti A MagdalenaNo ratings yet
- OctreotideDocument4 pagesOctreotideMihaela VișanNo ratings yet
- Stok 25mei23Document29 pagesStok 25mei23galihNo ratings yet
- Drug Study PediaDocument5 pagesDrug Study Pediajulesubayubay5428No ratings yet
- Unit 3 - Cology 3Document25 pagesUnit 3 - Cology 3Shreyas ShreyuNo ratings yet
- Amprahan Obat PustuDocument101 pagesAmprahan Obat Pustuyulinda purwantiNo ratings yet
- DiclofenacDocument56 pagesDiclofenacVikas Sharma0% (1)
- Drug InggrisDocument24 pagesDrug InggrisRewang LelosNo ratings yet
- Import Policy For Medicines. Govt of Pak (13-12-2013)Document2 pagesImport Policy For Medicines. Govt of Pak (13-12-2013)Mrs YezdaniNo ratings yet
- Insights Into Hypersensitivity Reactions In.6Document10 pagesInsights Into Hypersensitivity Reactions In.6rochmandrg dokter gigiNo ratings yet
- ImotilDocument2 pagesImotilMeraz AhmedNo ratings yet
- Danh Muc Co San Hang Hataphar 1Document6 pagesDanh Muc Co San Hang Hataphar 1Phương DungNo ratings yet
- D-Pharm-II Pharmaceutical Chemistry-II P-503Document4 pagesD-Pharm-II Pharmaceutical Chemistry-II P-503GSCSCL eAuction CellNo ratings yet
- AmoxicillinDocument9 pagesAmoxicillinShahd Diefalla Ahmed DiefallaNo ratings yet
- Self-Assessment Questions: Chapter 30: HypertensionDocument5 pagesSelf-Assessment Questions: Chapter 30: HypertensionRichix K YabeNo ratings yet
- Drug InfoDocument11 pagesDrug InfoArjun SinghNo ratings yet
- 10.beta Lactamase InhibitorsDocument15 pages10.beta Lactamase InhibitorsJagirNo ratings yet
- Saifur Rahman Sabbir Tika Card - Masum BestDocument1 pageSaifur Rahman Sabbir Tika Card - Masum BestTowhidul Azam BabuNo ratings yet