You might also like
- Sirgut Tesfaye Simulation ProjectDocument19 pagesSirgut Tesfaye Simulation ProjectSirgut TesfayeNo ratings yet
- Forecasting Emergency Department Crowding: A Prospective, Real-Time EvaluationDocument8 pagesForecasting Emergency Department Crowding: A Prospective, Real-Time EvaluationARTZchebilNo ratings yet
- A Hospital Capacity Planning Model: Darryl Gove and David HewettDocument4 pagesA Hospital Capacity Planning Model: Darryl Gove and David HewettMuchtar ZarkasyiNo ratings yet
- A Stochastic Optimization Model For Shift Scheduling in Emergency DepartmentsDocument19 pagesA Stochastic Optimization Model For Shift Scheduling in Emergency DepartmentsterrywangshimingNo ratings yet
- ###Annalsats 201409-419ocDocument9 pages###Annalsats 201409-419ocTawhid MahmudNo ratings yet
- 38 Hoot 2007Document9 pages38 Hoot 2007ARTZchebilNo ratings yet
- Modeling and Simulation of Patient Flow in Hospitals For Resource UtilizationDocument10 pagesModeling and Simulation of Patient Flow in Hospitals For Resource UtilizationIndra GunawanNo ratings yet
- A Simulation Study To Analyze The Impact of Different Emergency Physician Shift Structures in An Emergency DepartmentDocument8 pagesA Simulation Study To Analyze The Impact of Different Emergency Physician Shift Structures in An Emergency DepartmentBilal SalamehNo ratings yet
- Improving The Efficiency of A Hospital Emergency Department: A Simulation Study With Indirectly Imputed Service-Time DistributionsDocument28 pagesImproving The Efficiency of A Hospital Emergency Department: A Simulation Study With Indirectly Imputed Service-Time DistributionsashlyduartNo ratings yet
- Surgical Case Scheduling As A Generalized Job Shop Scheduling ProblemDocument15 pagesSurgical Case Scheduling As A Generalized Job Shop Scheduling ProblemRiya SharmaNo ratings yet
- Nese Colak Oray Sedat Yanturali Ridvan ATILLA Gurkan ERSOY Hakan Topacoglu Author Information Article NotesDocument17 pagesNese Colak Oray Sedat Yanturali Ridvan ATILLA Gurkan ERSOY Hakan Topacoglu Author Information Article Notesbro nawalibmatNo ratings yet
- Modeling The Emergency Cardiac In-Patient FlowDocument27 pagesModeling The Emergency Cardiac In-Patient FlowVibhu KesharwaniNo ratings yet
- Operation Theatre PerformanceDocument8 pagesOperation Theatre PerformancePriyanka SatalkarNo ratings yet
- Accepted Manuscript: Computer Methods and Programs in BiomedicineDocument26 pagesAccepted Manuscript: Computer Methods and Programs in BiomedicineRia AmeliaNo ratings yet
- Stochastic Programming For Outpatient Scheduling With Flexible Inpatient Exam AccommodationDocument23 pagesStochastic Programming For Outpatient Scheduling With Flexible Inpatient Exam Accommodationnancy.vargasNo ratings yet
- Hung 2007Document6 pagesHung 2007Sofia CamachoNo ratings yet
- SP00 02 PDFDocument7 pagesSP00 02 PDFBrianNo ratings yet
- Anticipating The Patient Emergency Data in Hospital Using Machine Learning AlgorithmDocument12 pagesAnticipating The Patient Emergency Data in Hospital Using Machine Learning AlgorithmbhasutkarmaheshNo ratings yet
- Emergency DepartmentDocument5 pagesEmergency Departmentsanjog DewanNo ratings yet
- Opd Paper33Document12 pagesOpd Paper33Anonymous wwYl2Pvt3rNo ratings yet
- Machine Learning Based Integrated Scheduling and Rescheduling For Elective and Emergency Patients in The Operating TheatreDocument24 pagesMachine Learning Based Integrated Scheduling and Rescheduling For Elective and Emergency Patients in The Operating Theatreayed latifaNo ratings yet
- SE Asignment PDFDocument20 pagesSE Asignment PDFSanam BirdiNo ratings yet
- Early Hospital Mortality Prediction Using Vital SignalsDocument11 pagesEarly Hospital Mortality Prediction Using Vital SignalsUday GulghaneNo ratings yet
- J Ajem 2021 04 075Document6 pagesJ Ajem 2021 04 075钟俊毅No ratings yet
- 2011 - Application of Queuing Theory in Health CareDocument11 pages2011 - Application of Queuing Theory in Health CareAneri JainNo ratings yet
- A Hospital Unit Performance CalculatorDocument15 pagesA Hospital Unit Performance CalculatorloloNo ratings yet
- Machine Learning Based Models To Support Decision Maki - 2021 - International JoDocument7 pagesMachine Learning Based Models To Support Decision Maki - 2021 - International JobasubuetNo ratings yet
- 36-Article Text-584-1-10-20200623Document11 pages36-Article Text-584-1-10-20200623Karin ClaveriasNo ratings yet
- Hospital Management SRSDocument11 pagesHospital Management SRSMohammed alraeyNo ratings yet
- Simulation ProjectDocument5 pagesSimulation ProjectDebasish Sarkar100% (1)
- J 1553-2712 2011 01122 X PDFDocument8 pagesJ 1553-2712 2011 01122 X PDFSriatiNo ratings yet
- Articulo CientificoDocument12 pagesArticulo CientificoAngeles Jiménez DuhartNo ratings yet
- Jurnal Code Blue PDFDocument4 pagesJurnal Code Blue PDFAfi Adi KiranaNo ratings yet
- Simulation Model For Patient Workflow at Selected Emergency Rooms During HajjDocument18 pagesSimulation Model For Patient Workflow at Selected Emergency Rooms During Hajjrabe ahmedNo ratings yet
- ED Crowding SolutionsDocument12 pagesED Crowding SolutionsFikriNo ratings yet
- Epstein & Tian, 2006Document6 pagesEpstein & Tian, 2006Nurul AidaNo ratings yet
- Healthcare 10 01518Document24 pagesHealthcare 10 01518ayed latifaNo ratings yet
- Application of Data Mining Techniques To Predict Length of Stay of Stroke PatientsDocument5 pagesApplication of Data Mining Techniques To Predict Length of Stay of Stroke Patientswisa arbiNo ratings yet
- Triage Critical Care ScoringDocument121 pagesTriage Critical Care ScoringAira LorenzoNo ratings yet
- Machine Learning For Clinical Outcome PredictionDocument11 pagesMachine Learning For Clinical Outcome PredictionhiimamanenuNo ratings yet
- An Improved Queuing Model For Reducing A PDFDocument14 pagesAn Improved Queuing Model For Reducing A PDFUzair KhanNo ratings yet
- Hoot2007 PDFDocument9 pagesHoot2007 PDFDaniel Peña BenavidesNo ratings yet
- Forecasting Hospital Bed Availability Using Simulation and Neural NetworksDocument6 pagesForecasting Hospital Bed Availability Using Simulation and Neural NetworksThiago PoeysNo ratings yet
- A Study On Process and Analysis of Opd Waiting Time in Phlebotomy AreaDocument29 pagesA Study On Process and Analysis of Opd Waiting Time in Phlebotomy AreaMiracle Online ServicesNo ratings yet
- An Improved Queuing Model For Reducing Average Waiting Time of Emergency Surgical Patients Using Preemptive Priority SchedulingDocument14 pagesAn Improved Queuing Model For Reducing Average Waiting Time of Emergency Surgical Patients Using Preemptive Priority SchedulingVelumani sNo ratings yet
- Hospital Management System RequirementsDocument9 pagesHospital Management System Requirementsvinod kapateNo ratings yet
- Shannon - YFT - EVD - Editors - Comments (Second Round)Document19 pagesShannon - YFT - EVD - Editors - Comments (Second Round)rabia khalidNo ratings yet
- s41598 021 98851 7Document19 pagess41598 021 98851 7Kumar palNo ratings yet
- 2 Minimizing The Waiting Time For Emergency SurgeryDocument11 pages2 Minimizing The Waiting Time For Emergency SurgeryFelix NainggolanNo ratings yet
- Optimization of An Appointment Scheduling ProblemDocument20 pagesOptimization of An Appointment Scheduling ProblemKumar palNo ratings yet
- Draft 3Document3 pagesDraft 3michealNo ratings yet
- Hybrid algorithm schedules surgeriesDocument33 pagesHybrid algorithm schedules surgerieshanaNo ratings yet
- SOFTWARE REQUIREMENTS HospDocument12 pagesSOFTWARE REQUIREMENTS HospAtsham AliNo ratings yet
- Indicator Standardized Mortality Rate (SMR) or Risk Adjusted Mortality RateDocument4 pagesIndicator Standardized Mortality Rate (SMR) or Risk Adjusted Mortality RatejeleksorminNo ratings yet
- Improving ICU Length of Stay Prediction Using Hidden Markov ModelsDocument10 pagesImproving ICU Length of Stay Prediction Using Hidden Markov ModelsTanvin AyatNo ratings yet
- ResearchDocument11 pagesResearchIMNG_PDFNo ratings yet
- A Stochastic Model For Operating Room PLDocument12 pagesA Stochastic Model For Operating Room PLlonely.jugiezNo ratings yet
- Case ReportDocument5 pagesCase ReportrizkaaslamNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
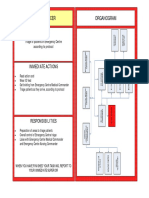
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- February 11, 2011 Strathmore TimesDocument24 pagesFebruary 11, 2011 Strathmore TimesStrathmore TimesNo ratings yet
- Google LensDocument1 pageGoogle Lenstamo.chilingarashviliNo ratings yet
- 3 EHSTG Assessment Hand Book Revised June 2018Document83 pages3 EHSTG Assessment Hand Book Revised June 2018Siham Si Seid100% (5)
- Hospital Admission Form GuideDocument6 pagesHospital Admission Form GuideAthiaNo ratings yet
- COVIDSurg-Cancer AuthorshipDocument33 pagesCOVIDSurg-Cancer AuthorshiphamishNo ratings yet
- Dr. Michael Banks License RevocationDocument69 pagesDr. Michael Banks License RevocationWKYC.comNo ratings yet
- OP IP Network - IRIS FortuneDocument88 pagesOP IP Network - IRIS FortunehamzadarbarNo ratings yet
- Chennai Bus RoutesDocument69 pagesChennai Bus RoutesAakash SrivastavaNo ratings yet
- Alimannao Hills, Peñablanca, Cagayan E-Mail Address: Adminoffice@isap - Edu.phDocument3 pagesAlimannao Hills, Peñablanca, Cagayan E-Mail Address: Adminoffice@isap - Edu.phmark OrpillaNo ratings yet
- Organizational ChartDocument1 pageOrganizational ChartQueeny Anne Apil0% (1)
- Resident Handbook 06.30.21Document44 pagesResident Handbook 06.30.21Salim MichaelNo ratings yet
- Old Age Home DesignDocument6 pagesOld Age Home DesignRaj Kumar67% (6)
- Modern Healthcare Delivery, Deliverance or Debacle - A Glimpse From The Inside OutDocument6 pagesModern Healthcare Delivery, Deliverance or Debacle - A Glimpse From The Inside OutMichael J Zema MDNo ratings yet
- Community Voices For Health System Accountability LetterDocument4 pagesCommunity Voices For Health System Accountability LetterJonathan LaMantiaNo ratings yet
- Hubungan Disiplin Dan Beban Kerja Dengan Kinerja Perawat Di Ruang Rawat Inap Rumah Sakit Umum Daerah (Rsud) Undata PaluDocument10 pagesHubungan Disiplin Dan Beban Kerja Dengan Kinerja Perawat Di Ruang Rawat Inap Rumah Sakit Umum Daerah (Rsud) Undata PaluNur Aeni777No ratings yet
- Application LetterDocument1 pageApplication LetterWetzell PornelNo ratings yet
- Elutax PosterDocument1 pageElutax PosterAlexander RuebbenNo ratings yet
- Reducing Readmissions Through Follow-Up Appointments - RPI Project Charter - Readmissions - TOOL 2 of 3Document1 pageReducing Readmissions Through Follow-Up Appointments - RPI Project Charter - Readmissions - TOOL 2 of 3eman hamzaNo ratings yet
- Jurnal Kinerja PerawatDocument5 pagesJurnal Kinerja PerawatErvie KochetzNo ratings yet
- Moh. Ilham Firdaus (1019031083) Psik 2B Asking and Showing Rooms in HospitalDocument4 pagesMoh. Ilham Firdaus (1019031083) Psik 2B Asking and Showing Rooms in HospitalFadilah Anjar MastrinNo ratings yet
- Waring 2019Document20 pagesWaring 2019Alexander GombergNo ratings yet
- NICU TRAINING PROPOSAL- finalDocument3 pagesNICU TRAINING PROPOSAL- finalJohn Troy GamilNo ratings yet
- Student's Book Unit 5Document10 pagesStudent's Book Unit 5Pau FlurscheimNo ratings yet
- Assam and NE Tie UpDocument1 pageAssam and NE Tie UpsureesicNo ratings yet
- Work Immersion Place HistoryDocument2 pagesWork Immersion Place HistoryRichmond Lloyd Menguito JavierNo ratings yet
- Fake Nurse ResumeDocument2 pagesFake Nurse Resumeapi-657085993No ratings yet
- MGT 489 Final Exam Submission Document: Section: 18 Student Name: Samrin HassanDocument8 pagesMGT 489 Final Exam Submission Document: Section: 18 Student Name: Samrin HassanSamrin HassanNo ratings yet
- Vancouver Coastal Health Facilities That Declared "Enhanced Surveillance" Status After A Covid-19 Infection: VCH 2021-F-019 Responsive RecordDocument1 pageVancouver Coastal Health Facilities That Declared "Enhanced Surveillance" Status After A Covid-19 Infection: VCH 2021-F-019 Responsive RecordIan YoungNo ratings yet
- Ahemadnagaar CentresDocument32 pagesAhemadnagaar CentresDhruv VasudevaNo ratings yet