You might also like
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Basileus Training Presentation 2020Document19 pagesBasileus Training Presentation 2020heru nurudinNo ratings yet
- English Words From Latin and Greek Roots A Dictionary of Latin and Greek Roots in English Vocabulary (Abhinav Kushwaha)Document110 pagesEnglish Words From Latin and Greek Roots A Dictionary of Latin and Greek Roots in English Vocabulary (Abhinav Kushwaha)genie redNo ratings yet
- 347-Let All Mortal Flesh Keep SilenceDocument1 page347-Let All Mortal Flesh Keep SilenceGarrett KheshtinejadNo ratings yet
- Math 12 ABM BESR Q1 Week 6Document16 pagesMath 12 ABM BESR Q1 Week 6AÑORA, Princess Aeyah M.No ratings yet
- Headway Test Unit 5ADocument3 pagesHeadway Test Unit 5Akaro2511personalNo ratings yet
- Powders and Granules For Syrups: Nasal PreparationsDocument2 pagesPowders and Granules For Syrups: Nasal PreparationsAat Prayoga MuhtarNo ratings yet
- 2017 Grade 7 Math Challenge Elimination QuestionsDocument2 pages2017 Grade 7 Math Challenge Elimination QuestionsOwen CajarteNo ratings yet
- MCQs Basic Statistics 1Document6 pagesMCQs Basic Statistics 1secret student100% (1)
- After Sales ServiceDocument4 pagesAfter Sales ServiceDan John KarikottuNo ratings yet
- Proporcion Aurea DebussyDocument6 pagesProporcion Aurea DebussyTomás Grau BaenaNo ratings yet
- Emergency Trolley (Abc) ChecklistDocument64 pagesEmergency Trolley (Abc) ChecklistN.K. Ayu SuksmawatiNo ratings yet
- Checklist-Audit Troli KecemasanDocument4 pagesChecklist-Audit Troli Kecemasanjzarizi100% (6)
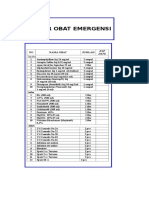
- Daftar Obat Alkes Trolley EmergencyDocument15 pagesDaftar Obat Alkes Trolley EmergencyPRIHATINNo ratings yet
- Daftar Perlengkapan Medis Ambulan Gawat DaruratDocument2 pagesDaftar Perlengkapan Medis Ambulan Gawat DaruratNurul PatrisiaNo ratings yet
- Test Bank For The Real World 6th Edition Kerry Ferris Jill SteinDocument10 pagesTest Bank For The Real World 6th Edition Kerry Ferris Jill Steinload.notablewp0oz100% (34)
- Lista Produselor 2-8 CDocument5 pagesLista Produselor 2-8 Cadelina78100% (3)
- Daftar Obat Alkes Trolley EmergencyDocument15 pagesDaftar Obat Alkes Trolley EmergencyiraNo ratings yet
- Instrument DetailsDocument2 pagesInstrument DetailsDebabrata MajhiNo ratings yet
- Transport Media & Swabs: Three Types of MediaDocument6 pagesTransport Media & Swabs: Three Types of MediaPankaj WaghNo ratings yet
- Chlorine HR PP M111 0.1 - 8 MG/L CL CL8 DPD: Instrument Specific InformationDocument10 pagesChlorine HR PP M111 0.1 - 8 MG/L CL CL8 DPD: Instrument Specific Informationcristi5cNo ratings yet
- First Aid Box ContentsDocument1 pageFirst Aid Box ContentsReaz UddinNo ratings yet
- Stok Tetap Ruang Anak NO Nama Perbekalan Farmasi Satuan JumlahDocument4 pagesStok Tetap Ruang Anak NO Nama Perbekalan Farmasi Satuan JumlahSarah AlmiraNo ratings yet
- Kebutuhan Alkes & Obat Ruang Igd 2019: Alkes Ukuran Jumlah Keterangan CairanDocument5 pagesKebutuhan Alkes & Obat Ruang Igd 2019: Alkes Ukuran Jumlah Keterangan CairanRania PutriNo ratings yet
- DLAB Manual-Pipettes Micropipette-Plus ManualDocument20 pagesDLAB Manual-Pipettes Micropipette-Plus ManualMax MustermannNo ratings yet
- Dräger Babyflow Plus Consumables and AccessoriesDocument6 pagesDräger Babyflow Plus Consumables and AccessoriesDigaimedicNo ratings yet
- REKAP BMHP Masih KosongDocument8 pagesREKAP BMHP Masih KosongArip AiluaNo ratings yet
- 3.1.4 Immobilised Enzymes ExpDocument3 pages3.1.4 Immobilised Enzymes ExpNazliNo ratings yet
- Panduan Troli EmergencyDocument3 pagesPanduan Troli EmergencyTukiyemNo ratings yet
- Guaifenesin Flemaxir Guaifenesin Flemaxir: Expectorant ExpectorantDocument1 pageGuaifenesin Flemaxir Guaifenesin Flemaxir: Expectorant ExpectorantKaela LizadoNo ratings yet
- 10.4 EmergencyTrolley Checklist CHCDocument4 pages10.4 EmergencyTrolley Checklist CHCAlisha AguetNo ratings yet
- Venomil Dilution ChartsDocument2 pagesVenomil Dilution ChartsAndrej KazancevNo ratings yet
- Genericsking Trading Inc Ampules Vials 1 WholesaleDocument12 pagesGenericsking Trading Inc Ampules Vials 1 Wholesaleapi-276695824No ratings yet
- Catálogo Gerber Cap-LabDocument83 pagesCatálogo Gerber Cap-LabJocilene Dantas Torres NascimentoNo ratings yet
- Daftar Obat Alkes Trolley EmergencyDocument15 pagesDaftar Obat Alkes Trolley EmergencydevitaNo ratings yet
- Troli KecemasanDocument4 pagesTroli KecemasanSUHANA TUMINNo ratings yet
- Form Standarisasi BMHP RSU Jampang Kulon 2020Document6 pagesForm Standarisasi BMHP RSU Jampang Kulon 2020Avrilia Fuji AstutiNo ratings yet
- Finnpipette F3 ManualDocument24 pagesFinnpipette F3 ManualUjang KarnaNo ratings yet
- Crash CartDocument2 pagesCrash CartKomal Tomar100% (1)
- AxyPrep DNA Gel Extraction KitDocument6 pagesAxyPrep DNA Gel Extraction Kitwaqas rafiqueNo ratings yet
- Model 475 Gradient Delivery System Instruction Manual: Catalog Number 170-9042Document15 pagesModel 475 Gradient Delivery System Instruction Manual: Catalog Number 170-9042y913708No ratings yet
- Requerimiento de Material de Consumo LaboratorioDocument3 pagesRequerimiento de Material de Consumo LaboratorioJuan Carlos Montoya GuzmánNo ratings yet
- Fuel Testing ConsumablesDocument2 pagesFuel Testing Consumablesshy_boyNo ratings yet
- Intubation Set Qty. Intubation Set QtyDocument1 pageIntubation Set Qty. Intubation Set QtyJaypee Fabros EdraNo ratings yet
- Product List in PDFDocument8 pagesProduct List in PDFManoj SolankiNo ratings yet
- Edit Lplpo 2020Document11 pagesEdit Lplpo 2020fiftha agustinaNo ratings yet
- Data Obat Agustus 2016Document195 pagesData Obat Agustus 2016Sri WahyuningsihNo ratings yet
- Daftar Jenis AlkesDocument2 pagesDaftar Jenis AlkesMuhammad MukhlisNo ratings yet
- Ambulance ChecklistDocument43 pagesAmbulance ChecklistRatnaSuryatiNo ratings yet
- Lplpo EndangDocument129 pagesLplpo Endangdaria derma clinicNo ratings yet
- DAFTAR OBAT Ruang ISOLASIDocument1 pageDAFTAR OBAT Ruang ISOLASIayu amaliaNo ratings yet
- Housekeeping InventoryDocument1 pageHousekeeping InventoryBatu Indah Pool VillaNo ratings yet
- 4551-3a Bio Pat F4 2014Document15 pages4551-3a Bio Pat F4 2014achik_aliezNo ratings yet
- Eppendorf Liquid-Handling Brochure Multipette-M4 Count-ItDocument6 pagesEppendorf Liquid-Handling Brochure Multipette-M4 Count-ItIgor de OliveiraNo ratings yet
- Daftar Trolley EmgDocument5 pagesDaftar Trolley EmgmutiaNo ratings yet
- Fix RK BMHP, Reagen, Bahan Gigi 2021 Untuk PKM 2Document13 pagesFix RK BMHP, Reagen, Bahan Gigi 2021 Untuk PKM 2laboratorium biatanNo ratings yet
- List Box Emergency IcuDocument2 pagesList Box Emergency IcuTedi UsNo ratings yet
- Anae Series CatalogDocument4 pagesAnae Series CatalogGerda CandraNo ratings yet
- KI Ophthal Dossier Status WHO GMPDocument8 pagesKI Ophthal Dossier Status WHO GMPGautam ShahNo ratings yet
- Eye Drops Eye Drops: DI 9FFTR731 DI 9FFTR731Document1 pageEye Drops Eye Drops: DI 9FFTR731 DI 9FFTR731mystery brainNo ratings yet
- Food Microbiology Sampling and PlatingDocument8 pagesFood Microbiology Sampling and PlatingThảo NguyễnNo ratings yet
- Alat Habis Pakai Hcu 2015 Alat Habis Pakai Hcu 2015 Rs 'Aisyiyah' Siti Fatimah Tulangan Sidoarjo Rs 'Aisyiyah' Siti Fatimah Tulangan SidoarjoDocument2 pagesAlat Habis Pakai Hcu 2015 Alat Habis Pakai Hcu 2015 Rs 'Aisyiyah' Siti Fatimah Tulangan Sidoarjo Rs 'Aisyiyah' Siti Fatimah Tulangan SidoarjoKritez DovecNo ratings yet
- No Produk Keterangan HargaDocument1 pageNo Produk Keterangan HargaIndriani Putri MardiyahNo ratings yet
- Buccal Smear Lab ReportDocument6 pagesBuccal Smear Lab ReportAugustNo ratings yet
- Tube O DIALYZER: No Loss Dialyzer For Small Samples (Cat. # 786 610 To 786 624)Document12 pagesTube O DIALYZER: No Loss Dialyzer For Small Samples (Cat. # 786 610 To 786 624)SergeyNo ratings yet
- AIESEC Way External Communication GuideDocument25 pagesAIESEC Way External Communication GuideSneha BalaaNo ratings yet
- CANINE-Canine Hepatozoonosis-Pathophysiology, Diagnosis and TreatmentDocument10 pagesCANINE-Canine Hepatozoonosis-Pathophysiology, Diagnosis and Treatmenttaner_soysuren0% (1)
- TEMPLATE-ACCOMPLISHMENT-REPORT-DRY-RUN-DISTRIBUTION-AND-RETRIVAL-Reyes, Rea C.Document7 pagesTEMPLATE-ACCOMPLISHMENT-REPORT-DRY-RUN-DISTRIBUTION-AND-RETRIVAL-Reyes, Rea C.Ma'am Rea Seyer100% (4)
- 21st REVIEWER 1ST SEM.Document4 pages21st REVIEWER 1ST SEM.janline bedicoNo ratings yet
- Essay 1201 Viva La Vida 1Document4 pagesEssay 1201 Viva La Vida 1api-509629411No ratings yet
- Book of TobitDocument13 pagesBook of TobitAgent 47No ratings yet
- The Role of MonarchDocument15 pagesThe Role of MonarchPhạm ĐăngNo ratings yet
- WhatsApp Use in A Higher Education Learning EnviroDocument15 pagesWhatsApp Use in A Higher Education Learning Envirotampala weyNo ratings yet
- Assailed in This Petition For Review On Certiorari Under Rule 45 of The Rules of Court Is The DecisionDocument22 pagesAssailed in This Petition For Review On Certiorari Under Rule 45 of The Rules of Court Is The DecisionCris Margot LuyabenNo ratings yet
- Factors of Causes of Deviation in TafsirDocument14 pagesFactors of Causes of Deviation in Tafsirfatkhul mubinNo ratings yet
- INF1511 - Chapter 4 - Functions and ModulesDocument3 pagesINF1511 - Chapter 4 - Functions and ModulesRofhiwa RamahalaNo ratings yet
- Riverhead High School NJROTC 2013 Awards Dinner ProgramDocument5 pagesRiverhead High School NJROTC 2013 Awards Dinner ProgramRiverheadLOCALNo ratings yet
- Women's Expectations From Delivery Nurses of Vaginal Birth: A Qualitative StudyDocument9 pagesWomen's Expectations From Delivery Nurses of Vaginal Birth: A Qualitative Studykaycelyn jimenezNo ratings yet
- Name: Kristel Rose S. Pasaol Beed 4: ACTIVITY - Let's Read These Observation Guide For The Learner's Social BehaviorDocument7 pagesName: Kristel Rose S. Pasaol Beed 4: ACTIVITY - Let's Read These Observation Guide For The Learner's Social BehaviorfgjxxiNo ratings yet
- The Tavistock Learning Group - Exploration Outside The Traditional FrameDocument287 pagesThe Tavistock Learning Group - Exploration Outside The Traditional FrameNicolás BerasainNo ratings yet
- Expert Systems Principles and Programming Third Edition PDFDocument2 pagesExpert Systems Principles and Programming Third Edition PDFRebecca0% (1)
- MAD Art of Caricatures by Tom Richmond Do WordDocument192 pagesMAD Art of Caricatures by Tom Richmond Do WordJjaz Animações ZíporaNo ratings yet
- QuantifiersDocument4 pagesQuantifiersKevin WindellNo ratings yet
- Gaining Access, Developing Trust, Acting Ethically 7Document31 pagesGaining Access, Developing Trust, Acting Ethically 7Bisma NazirNo ratings yet
- Chytidiomycoya: Blastocladiales Neocallimasticales Monoblepbaridales Chytridiales SpizellomycetalesDocument7 pagesChytidiomycoya: Blastocladiales Neocallimasticales Monoblepbaridales Chytridiales Spizellomycetalesratih purwaningrum13No ratings yet