Professional Documents
Culture Documents
Childhood ALL KET HOP
Uploaded by
Do Cam TunCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Childhood ALL KET HOP
Uploaded by
Do Cam TunCopyright:
Available Formats
VOLUME 33 䡠 NUMBER 27 䡠 SEPTEMBER 20 2015
JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E
Childhood Acute Lymphoblastic Leukemia: Progress
Through Collaboration
Ching-Hon Pui, Jun J. Yang, Stephen P. Hunger, Rob Pieters, Martin Schrappe, Andrea Biondi, Ajay Vora,
André Baruchel, Lewis B. Silverman, Kjeld Schmiegelow, Gabriele Escherich, Keizo Horibe, Yves C.M. Benoit,
Shai Izraeli, Allen Eng Juh Yeoh, Der-Cherng Liang, James R. Downing, William E. Evans, Mary V. Relling,
and Charles G. Mullighan
Author affiliations appear at the end of
this article. A B S T R A C T
Published online ahead of print at Purpose
www.jco.org on August 24, 2015. To review the impact of collaborative studies on advances in the biology and treatment of acute
Supported in part by Grants No. lymphoblastic leukemia (ALL) in children and adolescents.
CA21765, CA36401, U01 GM92666,
U10 CA98543 (to the Children’s Oncol- Methods
ogy Group [COG] Chair), and U10 A review of English literature on childhood ALL focusing on collaborative studies was
CA98413 (to the COG Statistical performed. The resulting article was reviewed and revised by the committee chairs of the
Center) from the National Institutes of
major ALL study groups.
Health; by the United Kingdom Medical
Research Council, Leukaemia and Results
Lymphoma Research and National With long-term survival rates for ALL approaching 90% and the advent of high-resolution
Cancer Research Institute (United King-
genome-wide analyses, several international study groups or consortia were established to
dom Childhood Acute Lymphoblastic
Leukemia trials); by a Stand Up to
conduct collaborative research to further improve outcome. As a result, treatment strategies have
Cancer Innovative Research Grant been improved for several subtypes of ALL, such as infant, MLL-rearranged, Philadelphia
(C.G.M.); by the Singapore VIVA Foun- chromosome–positive, and Philadelphia chromosome–like ALL. Many recurrent genetic abnormal-
dation; and by the American Lebanese ities that respond to tyrosine kinase inhibitors and multiple genetic determinants of drug
Syrian Associated Charities. S.P.H. is resistance and toxicities have been identified to help develop targeted therapy. Several genetic
the Ergen Family Chair in Pediatric
polymorphisms have been recognized that show susceptibility to developing ALL and that help
Cancer, C.G.M. is a St Baldrick’s
Scholar and Pew Scholar in the
explain the racial/ethnic differences in the incidence of ALL.
Biomedical Sciences, and C.-H.P. is an
Conclusion
American Cancer Society professor.
The information gained from collaborative studies has helped decipher the heterogeneity of ALL
Authors’ disclosures of potential to help improve personalized treatment, which will further advance the current high cure rate and
conflicts of interest are found in the the quality of life for children and adolescents with ALL.
article online at www.jco.org. Author
contributions are found at the end of
this article.
J Clin Oncol 33:2938-2948. © 2015 by American Society of Clinical Oncology
Corresponding author: Ching-Hon Pui,
MD, St Jude Children’s Research resistant leukemia, and they require concerted
INTRODUCTION
Hospital, 262 Danny Thomas Place, efforts by multiple study groups to identify effec-
Memphis, TN 38105; e-mail: ching-hon
.pui@stjude.org.
Remarkable progress has been made in the treat- tive treatment strategies. Parallel to the therapeu-
ment of childhood acute lymphoblastic leukemia tic gain have been the major advances in our
© 2015 by American Society of Clinical
Oncology (ALL) in the past two decades, with the propor- knowledge of leukemic cell biology, especially
0732-183X/15/3327w-2938w/$20.00 tion of patients surviving for 5 years approaching with the recent advent of genome-wide analysis.15
DOI: 10.1200/JCO.2014.59.1636
and even exceeding 90% in many developed Genome-wide studies to identify inherited and
countries (Table 1).1-14 Improved outcome can be somatically acquired genomic variations that in-
attributed to the optimal risk-directed therapy fluence disease incidence, treatment response, or
that incorporates delayed intensification with toxicities also require a large number of patients
vincristine, asparaginase, and dexamethasone; for discovery and validation studies and to adjust
high dose or escalating dose of methotrexate; and for the ancestral composition of study cohorts.
early use of intrathecal therapy. These treatment Indeed, many recent advances in genomics have
components were primarily established by the also been the results of national and, in many
randomized clinical trials performed by major co- instances, international collaborations. We high-
operative study groups. With the improved cure light here some of the major accomplishments
rates, current research efforts have focused in- resulting from these collaborations and point to
creasingly on small subsets of patients with drug- ongoing efforts for further advances.
2938 © 2015 by American Society of Clinical Oncology
Childhood ALL: Progress Through Collaboration
Table 1. Patient Characteristics and Treatment Results From Selected Clinical Trials
5-Year Cumulative Rate
No. of Age Range T-Cell of Isolated CNS 5-Year EFS 5-Year Overall
Study Group Years of Study Patients (years) ALL (%) Relapse (% ⫾ SE) (% ⫾ SE) Survival (% ⫾ SE) Reference
AIEOP-95 1995-2000 1,743 0-18 11 1.2 ⫾ 0.3 75.9 ⫾ 1.0 85.5 ⫾ 0.8 Conter et al1
BFM-95 1995-1999 2,169 0-18 13 1.8 ⫾ 0.3 79.6 ⫾ 0.9 87.0 ⫾ 0.7 Möricke et al2
CoALL-97 1997-2003 667 1-18 14 4.0 ⫾ 0.8 76.7 ⫾ 1.7 85.4 ⫾ 1.4 Escherich et al3
COG 2000-2005 7,153 0-21 7 NA NA 90.4 ⫾ 0.5 Hunger et al4
DCOG-9 1997-2004 859 1-18 11 2.6 ⫾ 0.6 80.6 ⫾ 1.4 86.4 ⫾ 1.2 Veerman et al5
DFCI 00-01 2000-2004 492 1-18 11 NA 80.0 ⫾ 2 91 ⫾ 1 Vrooman et al6
EORTC-CLG 1998-2008 1,947 1-18 15.2 1.7 ⫾ 0.3 82.7 ⫾ 0.9 89.7 ⫾ 0.7 Domenech et al7
IC-BFM 2002 2002-2007 5,060 1-18 13.3 1.9 ⫾ 0.1 74 ⫾ 1 82 ⫾ 1 Stary et al8
JCCLSG ALL 2000 2000-2004 305 1-15 9.8 0.9 ⫾ 0.1 79.7 ⫾ 2.4 89.2 ⫾ 1.8 Yamaji et al9
Ma-Spore ALL 2003 2002-2011 556 0-18 8.8 1.4 80.6 ⫾ 3.5 89.2 ⫾ 2.7 Yeoh et al10
MRC UKALL 2003 2003-2011 3,126 1-25 12 1.9 ⫾ 0.6 87.3 ⫾ 1.4 91.6 ⫾ 1.2 Vora et al11
NOPHO-2000 2002-2007 1,023 1-15 11 2.7 ⫾ 0.6 79.4 ⫾ 1.5 89.1 ⫾ 1.1 Schmiegelow et al12
SJCRH XV 2000-2007 498 1-18 15 2.7 ⫾ 0.8 87.3 ⫾ 2.9 93.5 ⫾ 1.9 Pui et al13
TPOG 1999-2010 152 0-18 7.2 1.4 ⫾ 1.0 84.2 ⫾ 3.0 90.2 ⫾ 2.4 Liu et al14
Abbreviations: AIEOP, Associazione Italiana di Ematologia Pediatrica; ALL, acute lymphoblastic leukemia; BFM, Berlin-Frankfurt-Münster; CoALL, Cooperative ALL (study group);
COG, Children’s Oncology Group; DCOG, Dutch Children’s Oncology Group; DFCI, Dana-Farber Cancer Institute (consortium); EFS, event-free survival; EORTC-CLG, European
Organisation for Research and Treatment of Cancer-Children’s Leukemia Group; IC-BFM, Intercontinental BFM; JCCLSG, Japanese Children’s Cancer and Leukemia Study Group;
Ma-Spore, Malaysia-Singapore; MRC UKALL, Medical Research Council United Kingdom Acute Lymphoblastic Leukemia; NA, not available; NOPHO, Nordic Society of Pediatric
Hematology and Oncology; SJCRH, St Jude Children’s Research Hospital; TPOG, Taiwan Pediatric Oncology Group.
tional Study and Multicentre, Randomised Trial in Infants Younger
INTERNATIONAL COLLABORATIVE STUDY GROUPS
Than 1 Year With Acute Lymphoblastic Leukaemia), which enrolled
482 infants age 0 to 12 months between 1999 and 2005 to investigate
The Ponte di Legno group, named after the site of the first major
the efficacy of a hybrid treatment regimen with elements for treating
meeting, was formed in 1995,16 has since been joined by 15 major
both ALL and acute myeloid leukemia.21 The study achieved a 4-year
study groups or institutions, and has held 14 working group meet-
event-free survival of 47.0% and overall survival of 55.3%, outcomes
ings.17 The participants agreed to use the same or similar criteria to
better than those achieved with most previous protocols but showing
present the treatment outcome so that results could be compared
no benefit from delayed-intensification therapy with high-dose cytar-
among various clinical trials to identify effective treatment strategies
abine and methotrexate. The current study, Interfant-06 (NCT00550992:
for specific subsets of ALL. The first series of 12 articles on long-term
results of clinical trials was published in Leukemia in 2000, and the International Collaborative Treatment Protocol for Infants Under One
second series of 15 articles was published in Leukemia in 2010.18 The Year With Acute Lymphoblastic or Biphenotypic Leukemia), assesses
group also studied challenging subsets of ALL, the key findings of early intensification with two blocks of acute myeloid leukemia induction
which are described in this review. therapy to improve outcome and examines the role of hematopoietic
Under the leadership of Haig Riehm and Giuseppe Masera, the stem-celltransplantationininfantsathighriskofrelapse(age⬍6months,
Berlin-Frankfurt-Münster (BFM) and the Associazione Italiana di MLL rearrangement, and initial leukocyte count ⱖ 300 ⫻ 109/L).22
Ematologia Pediatrica (AIEOP) study groups set an early example of To identify treatment components responsible for improved
fruitful international collaboration. Among their many collaborative treatment outcome, the Childhood ALL Collaborative Group was
studies, the two groups recently confirmed that minimal residual formed in 1994 to systematically review and analyze results from
disease (MRD) assessment is the most prognostic indicator in both B- relevant randomized trials. Analysis of data from four clinical trials
and T-cell ALL.19,20 They were also instrumental in developing the that enrolled patients between 1972 and 1984 showed that anthracy-
Intercontinental BFM (IC-BFM) Study Group comprising study clines reduced hematologic relapse but failed to improve event-free
groups from more than 30 countries worldwide to address therapeutic survival, partly because of the increased induction failures and deaths
questions tailored to their resources and technology. The IC-BFM in remission.23 Meta-analysis of trials started between 1965 and 1998
2002 (A Randomized Trial of the I-BFM-SG for Management of showed that the addition of vincristine plus prednisone or pred-
Childhood Non-B Acute Lymphoblastic Leukemia) study, which en- nisolone pulses during postremission therapy improved event-free
rolled 5,060 patients between 2002 and 2007 showed no significant survival; the lack of improvement with vincristine and dexamethasone
improvement in outcome with intensive or prolonged delayed- pulses in the more recent trials was attributed to the greater intensity of
intensification therapy, and it achieved a 5-year event-free survival of the early therapy.24 Meta-analysis of three trials that enrolled patients
74% and 5-year overall survival of 82%.8 Although the overall results between 1992 and 2002 suggested that thioguanine improved event-
were inferior to those of contemporaneous BFM studies because of the free survival compared with mercaptopurine for males younger than
high rate of treatment-related mortality, the national results have age 10 years, but its lack of effect on survival and association with a
generally improved and, importantly, this network demonstrated high risk of veno-occlusive disease of the liver made mercaptopurine
their ability to perform randomized clinical trials across continents. the standard thiopurine of choice.25 Meta-analysis of 47 trials of CNS-
Because of the rarity and distinct characteristics of infant ALL, 17 directed therapy conducted between 1970 and 1999 showed that
study groups collaborated on a clinical trial, Interfant-99 (Observa- CNS radiotherapy can generally be replaced by intrathecal therapy,
www.jco.org © 2015 by American Society of Clinical Oncology 2939
Pui et al
and triple intrathecal therapy should be used with effective sys- 11q23 abnormality conferred a dismal prognosis among infants,29 a find-
temic therapy such as intravenous high-dose methotrexate to real- ing confirmed by the Interfant-99 study.21 In the largest subgroup of
ize its full benefit of CNS control without the hazard of increased infants and children with t(4;11)(q21;q23), any type of transplantation,
systemic relapse.26 evenwithamatched-relateddonor,failedtoimproveoutcomecompared
Several working groups investigated the optimal use of asparagi- with chemotherapy alone.29 A separate analysis of the same cohort
nase. In one review, intensive use of asparaginase during the intensifi- showed that among patients with t(4;11)(q21;q23), infants fared signifi-
cation phase of therapy was credited for improved outcome.27 Two cantly worse than older patients.30 The Interfant-99 study showed that
studies showed improved outcome with therapeutic drug monitoring young age and MLL rearrangement independently predicted poor
during Escherichia coli asparaginase treatment; detection of silent in- outcome in infant ALL.21 Importantly, hematopoietic stem-cell
activation of the drug as a result of asparaginase antibody allowed for transplantation failed to improve the outcome of infants with MLL
early replacement with Erwinia asparaginase.6,28 rearrangement in the Interfant-99 study, with the exception of a
small subset of infants younger than age 6 months with either poor
CLINICAL ADVANCES IN SPECIFIC SUBTYPES OF ALL response to steroids or presenting leukocyte count ⱖ 300 ⫻ 109/L
who seemed to benefit from transplantation.22
Table 2 summarizes the findings of a few selected collaborative studies
that have had a major impact on clinical management. Hypodiploid ALL
The clinical and biologic characteristics of hypodiploid ALL have
ALL With 11q23 Rearrangement been poorly defined. In a study of 139 hypodiploid patients diagnosed
There is apparent clinical heterogeneity within each of the subtypes between 1986 and 1996, even after excluding nine patients with Phil-
of rearrangement of MLL at 11q23. In a study of 497 patients with 11q23 adelphia chromosome (Ph), the remaining 130 patients still had a
rearrangements diagnosed between 1983 and 1995, infants younger than poor outcome with an event-free survival of 38.3% at 8 years; inter-
1 year fared significantly worse than older patients, and any category of estingly, there were no induction failures, but information on the level
Table 2. Clinical Research Findings From Selected Collaborative Studies
No. of
Subgroup of Years Study No. of
ALL of Study Groups Patients Major Findings Reference
11q23 1983-1995 11 497 Prognosis was particularly dismal in infants; allogeneic transplantation did not Pui et al29,30
rearranged improve outcome in patients with t(4;11) ALL. Poor early response to
prednisone or age younger than 3 months conferred a particularly dismal
prognosis among infants with t(4;11).
Hypodiploid 1986-1996 11 139 Prognosis was very poor, especially among patients with fewer than 44 Nachman et al31
chromosomes.
Hypodiploid 2008-2013 2 126 Genome profiling and sequencing identifies distinct genetic alterations in Holmfeldt et al41
subtypes of hypodiploid ALL. Near-haploid patients have Ras pathway
mutations and IKZF3 mutations; low-hypodiploid patients have IKZF2
alterations and TP53 mutations, many of which are inherited.
Ph positive 1986-1996 10 326 Presenting age, leukocyte counts, and response to initial treatment with Aricò et al32
glucocorticoids and intrathecal methotrexate affected treatment outcome;
matched-related transplantation improved outcome.
Ph positive 1995-2005 10 610 Both matched-related and matched-unrelated transplantation improved Aricò et al33
treatment outcome.
Ph positive 2004-2009 10 178 Imatinib combined with intensive chemotherapy was well tolerated and might Biondi et al34
improve outcome.
Ph-like 2008-2009 2 221 Genetic alteration of IKZF1 was associated with high levels of minimal residual Mullighan et al35
disease and a very poor outcome.
Ph-like 2008-2009 2 297 These cases were associated with a high frequency of deletions in genes Den Boer et al36
involved in B-cell development, resistance to asparaginase and daunorubicin,
and unfavorable outcome.
Ph-like 2014 5 264 More than 90% of the patients had kinase-activating alterations, some of Roberts et al37
which were amenable to inhibition with tyrosine kinase inhibitors such as
imatinib or dasatinib.
Early T-cell 1992-2006 2 30 These patients had distinctive immunophenotype (CD1a⫺, CD8⫺, or CD5weak Coustan-Smith et al38
precursor with stem-cell or myeloid markers) and high risk of remission induction
failure or hematologic relapse.
Down syndrome 1995-2004 16 653 Compared with other patients, these patients have lower event-free survival as Buitenkamp et al39
a result of increased relapse hazard and treatment-related mortality. Younger
age and leukocyte count ⬍ 10 ⫻ 109/L at diagnosis and the presence of
high hyperdiploidy and ETV6-RUNX1 are favorable prognostic factors.
Induction failure 1985-2000 14 1,041 Patients with induction failure are highly heterogeneous. Although allogeneic Schrappe et al40
transplantation improved outcome for T-cell ALL, chemotherapy should be
the treatment of choice for B-ALL without other adverse features.
Abbreviations: ALL, acute lymphoblastic leukemia; Ph, Philadelphia chromosome.
2940 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Childhood ALL: Progress Through Collaboration
of MRD was not available.31 There were no significant differences in Early T-Cell Precursor ALL
outcome among patients with near haploidy (24 to 29 chromosomes), On the basis of gene expression profiling and flow cytometry, a
low hypodiploidy (33 to 39 chromosomes), or high hypodiploidy (40 collaborative study identified a distinct group of patients who repre-
to 43 chromosomes).31 Patients with fewer than 44 chromosomes sent approximately 12% of T-cell ALL with leukemia originating from
fared significantly worse than patients with 44 chromosomes, among a subset of thymocytes that retain a stem-cell–like feature.38 Although
whom those with monosomy 7, a dicentric chromosome, or both had the initial report showed that these patients had a high risk of remis-
a significantly worse event-free survival. There was no difference in sion induction failure or hematologic relapse,38 a recent study showed
outcome between patients with or without doubling of their hypodip- that they have intermediate-risk outcome (5-year event-free survival
loid clone. The efficacy of hematopoietic stem-cell transplantation of 76.7%) when treated with intensive chemotherapy, including dexa-
could not be adequately evaluated because only nine patients under- methasone and pegylated asparaginase.46
went this procedure.
Down Syndrome ALL
Ph-Positive ALL
Patients with Down syndrome who have ALL have inferior sur-
Before the development of ABL tyrosine kinase inhibitors, there
vival because of increased risk of relapse and treatment-related mor-
was no consensus on the optimal treatment of Ph-positive ALL. A
tality. The specific treatment phase responsible for increased death
combined study of 326 children and young adults diagnosed between
related to toxicity and the prognostic factors among these patients
1985 and 1996 disclosed a 5-year event-free survival (⫾ SE) of only
were not well characterized in previous small studies. In a large collab-
28% ⫾ 3% and that older age, high initial leukocyte count, and poor
orative study, these patients were found to have increased risk of
response to initial treatment with glucocorticoids and intrathecal
relapse, which tended to occur late, and to have increased treatment-
methotrexate adversely affected treatment outcome.32 Compared
related mortality throughout treatment, which resulted in lower
with chemotherapy alone, matched-related transplantation improved
event-free survival and overall survival but lower incidence of second-
outcome.32 A follow-up study of 610 patients diagnosed between 1995
ary malignancies compared with other children with ALL.39 Indepen-
and 2005 and treated without tyrosine kinase inhibitor showed that
dent favorable prognostic factors included age younger than 6 years,
the event-free survival had improved to 32% ⫾ 2% at 7 years, and both
leukocyte count less than 10 ⫻ 109/L, high hyperdiploidy, and ETV6-
matched-related and matched-unrelated transplantation improved
RUNX1 fusion. The lower rates of high hyperdiploidy (9% v 33%) and
outcome compared with chemotherapy alone.33 The results of this
ETV6-RUNX1 fusion (8% v 26%) than that found in other children
study served as a historical reference to the subsequent Children’s
may contribute partly to the increased risk of relapse in patients with
Oncology Group (COG) and European intergroup studies, showing
Down syndrome. The low rates of relapse among patients with Down
that postinduction imatinib mesylate plus intensive chemotherapy
syndrome with ETV6-RUNX1 fusion (3%) and especially those with
improved disease-free survival to 70% ⫾ 12% at 5 years and could
high hyperdiploidy and trisomies 4 and 10 (0%) suggested that treat-
spare patients with good initial response to remission induction from
ment reduction may be warranted for these subgroups of patients.39
transplantation.34,42 Whether dasatinib, a potent ABL tyrosine kinase
However, one study suggested that insufficient treatment intensity
inhibitor,43 given in conjunction with a BFM high-risk chemotherapy
during maintenance therapy (based on median WBC count) could
backbone can result in noninferior or improved outcome while reduc-
contribute to poor prognosis of patients with Down syndrome.47 A
ing the need for transplantation is being evaluated in a multicenter
Dutch Children’s Oncology Group (DCOG) study showed that the
study (NCT01460160: A Phase 2 Multi-Center, Historically Con-
IKZF1 deletion, which occurred in one third of patients with Down
trolled Study of Dasatinib Added to Standard Chemotherapy in Pedi-
syndrome, was a strong adverse prognostic factor.48 Because up to
atric Patients With Newly Diagnosed Philadelphia Chromosome
60% of patients with Down syndrome are Ph-like and are character-
Positive Acute Lymphoblastic Leukemia).
ized by CRLF2 overexpression and JAK-STAT activation, they may
potentially benefit from future therapy targeting kinase pathways.49,50
Ph-Like (BCR-ABL1–like) ALL
By using single nucleotide polymorphism microarrays, tran-
scriptional profiling, and gene resequencing, two group studies inde- ALL With Induction Failure
pendently identified a novel high-risk subtype of B-ALL that exhibits a Because induction failure occurs in only 2% to 3% of all patients,
gene expression profile similar to that of Ph-positive ALL with a high little was known about the heterogeneity among this group of patients
frequency of alterations of the IKZF1 gene but lacks the BCR-ABL1 who were generally offered allogeneic transplantation as the treatment
fusion protein.35,36 These patients were characterized by resistance of choice. In a large collaborative study, these patients, as expected,
to asparaginase and daunorubicin, a high level of MRD at the end were associated with older age, high leukocyte count, T-cell pheno-
of induction, and overall poor outcome.35,36 The BCR-ABL1–like type, Ph-positive ALL, and 11q23 chromosomal rearrangement.40
expression profile and IKZF1 deletions had independent poor Interestingly, although patients with T-cell ALL had improved out-
prognostic impact in a European collaborative study.44 Although come with matched-related transplantation, children younger than 6
risk-directed therapy, including intensive chemotherapy and allo- years with B-ALL and no other adverse genetic features had an excel-
geneic transplantation, could abolish the adverse prognostic signif- lent 10-year survival of 72% ⫾ 5% when treated with chemotherapy
icance of this genotype,45 a recent large collaborative study showed alone. The relatively favorable outcome of these patients with B-ALL
that a substantial proportion of patients have genomic alterations may be the result of increased sensitivity of the blast cells to metho-
that are amenable to inhibition with ABL tyrosine kinase inhibitors trexate and mercaptopurine, which are generally not used during
and potentially JAK inhibitors, which may spare some patients remission induction. Thus, this rare subset of patients with B-ALL
from transplantation.37 who readily achieve remission with subsequent consolidation therapy
www.jco.org © 2015 by American Society of Clinical Oncology 2941
Pui et al
with high-dose methotrexate and oral mercaptopurine could be activating mutations and deletions, including those involving IL7R,
spared from transplantation. FLT3, SH2B3, and others; and (5) infrequent targets of rearrangement
including NTRK3 and others. Patients with Ph-like ALL commonly
exhibit high-risk features and have a suboptimal response to ther-
BIOLOGIC ADVANCES
apy,36,37,45 and anecdotal reports are emerging of profound and lasting
response to the addition of tyrosine kinase inhibitors to patients with
Next-Generation Sequencing Studies Ph-like ALL with ABL1-class rearrangements.55,56 These findings have
Genome-wide studies have revolutionized our understanding led to prospective studies to identify Ph-like ALL (by low-density gene
of the genetic basis of ALL.51 These studies, using microarray
expression arrays and/or sequencing) and the underlying rearrange-
profiling of DNA copy number alterations and gene expression,
ments and to direct patients to logical kinase inhibitor therapy.
candidate gene sequencing and, more recently, second-generation
Early T-cell precursor ALL. By St Jude criteria, early T-cell pre-
sequencing (exome, transcriptome, and/or whole-genome se-
cursor (ETP) ALL is defined as a T-cell (cytoplasmic CD3⫹) leukemia
quencing), have resulted in three major advances: (1) revision of
that lacks expression of markers otherwise observed in T-cell ALL
the genetic subclassification of ALL by identifying new subtypes,
(CD1a, CD8, and weak and/or absent CD5) and has aberrant expres-
notably Ph-like, CRLF2-rearranged, ERG-deregulated, intrachro-
sion of myeloid or stem-cell markers.38 ETP ALL lacks a unifying
mosomal amplification of chromosome 21 (iAMP21), and early
chromosomal alteration,38 has a low frequency of genetic alterations
T-cell precursor ALL (Fig 1); (2) definition of the constellations of
otherwise common in T-ALL (eg, NOTCH1 mutations), and is
gross and submicroscopic structural genetic alterations and se-
quence mutations that characterize each ALL subtype; and (3) associated with MEF2C abnormalities in one European study.57
identification of genomic aberrations or profiles with diagnostic or One collaborative study of ETP ALL with whole-genome se-
prognostic implication (eg, IKZF1 alterations)35 or as targets for quencing identified frequent mutations in three pathways: hemato-
therapy (eg, kinase-activating alterations).37,45,52-54 Importantly, poietic development (eg, GATA3, IKZF1, RUNX1), cytokine receptor
these studies have enabled comprehensive genomic characteriza- and Ras signaling (eg, IL7R, NRAS, KRAS), and chromatin modifica-
tion of the three high-risk subtypes as described in this section. tion (eg, the polycomb repressor complex 2 and SETD2).58 Moreover,
IKZF1 alterations in high-risk B-ALL and Ph-like ALL. In 2009, human ETP ALL cells58 and a mouse model of Il7r-mutant ETP ALL59
two groups of investigators using a different gene expression profiling exhibit JAK-STAT activation that is inhibited by the JAK inhibitor
approach identified a subtype of high-risk B ALL that lacked a known ruxolitinib. These findings raise the prospect of targeted or pathway-
chromosomal rearrangement but exhibited a gene expression profile directed therapies, such as JAK inhibitors or epigenetic modifiers, to
similar to that of Ph-positive ALL with deletions and, less commonly, improve the outcome of ETP ALL.
sequence mutations of IKZF1.35,36 A recent study of this entity of Hypodiploid ALL. Until recently, the genetic basis for this high-
Ph-like or BCR-ABL1–like ALL showed that the prevalence increases risk hypodiploid ALL subtype has been poorly understood. A collab-
from 10% of standard-risk childhood ALL to more than one quarter orative study of 126 patients with hypodiploid ALL identified distinct
of young adult (age 21 to 39 years) ALL.37 The genetic basis of Ph-like submicroscopic alterations in each subtype.41 Patients with the near-
ALL is complex, including more than 30 rearrangements involving 13 haploid subtype had a high frequency of activating Ras pathway mu-
kinase, cytokine, or cytokine-receptor genes,37 but several key sub- tations (particularly novel deletions in NF1) and IKZF3 (Aiolos)
groups with therapeutic implications have been identified: (1) ABL- alterations, and patients with low-hypodiploid IKZF2 (Helios) muta-
class rearrangements targeting ABL1, ABL2, CSF1R, and PDGFRB, tions. A remarkable finding was the near universal presence of TP53
which are sensitive to imatinib and dasatinib; (2) EPOR and JAK2 mutations in low-hypodiploid ALL, which were in nontumor cells in
rearrangements sensitive to JAK inhibitors; (3) CRLF2 rearrange- more than half of patients and were shown to be inherited in a kindred
ments, frequently with concomitant activating JAK point mutations with other non-ALL tumors. Both near-haploid and low-hypodiploid
that may also be sensitive to JAK inhibition; (4) other JAK-STAT- leukemic cells had activation of the PI3K and Ras-Raf-MEK-ERK
A T-ALL ETP
1.2%
B ETP Hyperdiploid
12.6% T-ALL 6.3% 11.4%
Hyperdiploid 12.7%
28.2%
B-other
16.0% ETV6-RUNX1
21.5%
CRLF2 (not Ph-like) B-other
1.7% 20.3% Ph-like
MLL ETV6-RUNX1 3.8%
1.4% 18.6%
BCR-ABL1 CRLF2 (non-Ph-like)
1.7% Hypodiploid 1.3% MLL TCF3-PBX1
2.6% ERG 3.8% BCR-ABL1 ERG
3.1% TCF3-PBX1 Ph-like
8.8%
13.9%
4.1% 3.8% 1.3%
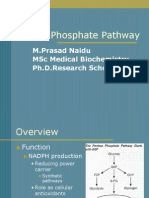
Fig 1. Estimated frequency of specific genotypes of childhood acute lymphoblastic leukemia (ALL) among patients treated in the St Jude Total Therapy Study XV.13
Genetic abnormalities among (A) all but black patients and (B) black patients who are more likely to have TCF3-PBX1 fusion and T-cell ALL (including early T-cell
precursor [ETP] ALL) but less likely to have hyperdiploidy. Ph, Philadelphia chromosome.
2942 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Childhood ALL: Progress Through Collaboration
signaling pathways, with sensitivity to PI3K/mTOR inhibitors, but not enced by common genetic variants. Recent advances in genome-wide
MEK inhibitors. These findings have important clinical implications: association studies (GWASs) substantially improved our understand-
patients with low-hypodiploid ALL should be tested for TP53 status to ing of genetic susceptibility to the development of childhood ALL.
enable appropriate surveillance and counseling, and preclinical stud- Because GWASs compare single nucleotide polymorphism genotypes
ies are evaluating the potential for PI3K and MEK inhibitors alone and across the whole genome between patients with ALL and non-ALL
in combination for hypodiploid ALL.
controls, hundreds or thousands of participants are required to obtain
robust results and to identify associations with ALL subtypes. Because
Inherited Genetic Determinants of Leukemogenesis
of the relatively rarity of childhood ALL, collaborative efforts are
Children with certain constitutional genetic abnormalities (eg,
trisomy 21) are at increased risk of developing ALL, and inherited almost always needed for these studies. In 2009, two independent
mutations in TP53 and PAX5 have also been described recently in studies described ARID5B and IKZF1 as loci having the strongest
familial (as well as sporadic) ALL.41,60 However, the vast majority of association with the risk of developing ALL.61,62 A subsequent collab-
childhood ALL occurences are not explained by these predisposing orative study using meta-analysis identified yet another susceptibility
genetic abnormalities; instead, disease susceptibility is mainly influ- locus at the CDKN2A/CDKN2B locus.63 A recent GWAS by St Jude
Table 3. Genome-Wide Association of Studies of Susceptibility of Childhood ALL
Study Group and Location Study Population Sample Size Susceptibility Loci OR 95% CI Comment Reference
COG, SJCRH Europeans 441 ARID5B (rs10821936) 1.91 1.6 to 2.2 ARID5B SNP discriminated Treviño et al61
IKZF1 (rs11978267) 1.69 1.4 to 1.9 hyperdiploid ALL from
other subtypes of ALL
and was associated with
accumulation of
methotrexate
polyglutamates.
UKCCS, MRC Europeans 907 ARID5B (rs7089424) 1.65 1.5 to 1.7 ARID5B variant was over- Papaemmanuil
IKZF1 (rs4132601) 1.69 1.5 to 1.8 represented in et al62
hyperdiploid ALL.
CEBPE (rs2239633) 1.34 1.2 to 1.4
UK, BFM, Spain, Hungary, Europeans and European 3,293 ARID5B CDKN2A encoded both p16 Sherborne
Canada Canadians IKZF1 and p14 and was et al63
associated with the
CEBPE
development of both B-
CDKN2A (rs3731217) 0.71 0.6 to 07 and T-ALL.
COG, SJCRH European Americans, African 2,450 ARID5B (rs10821936) 1.86 1.7 to 2.0 ARID5B, BMI1-PIP4K2A, Xu et al64
Americans, Hispanic IKZF1 (rs11978267) 1.59 1.4 to 1.7 and IKZF1 associations
Americans were consistent across
CEBPE (rs4982731) 1.36 1.2 to 1.4
ethnicity, and the
CDKN2A 1.36 1.1 to 1.5 frequencies of the
(rs17756311) ARID5B and BMI1-
PIP4K2A (rs7088318) 1.40 1.2 to 1.5 PIP4K2A variants differed
BMI1 (rs4748793) 1.40 1.2 to 1.5 in parallel with the ethnic
differences in ALL
incidence. These variants
independently and
cumulatively contribute
to ALL risk.
AIEOP, BFM, CoALL Europeans 1,370 TP63 (rs17505102) 0.63 0.5 to 0.7 In addition to IKZF1, DDC, Ellinghaus et
PTPRJ (rs3942852) 0.77 0.6 to 0.8 ARID5B, and CEBPE, al66
variants in TP63 (a
member of the TP53
gene family) and PTPRJ
(a receptor type protein
tyrosine phosphatase)
were associated with
ETV6-RUNX1 ALL.
COG, SJCRH Americans of different 682 GATA3 (rs3824662) 3.85 2.7 to 5.4 GATA3 was associated with Perez-Andreu
ancestry Ph-like ALL and risk of et al67
ALL relapse.
UKCCS, MRC UKALL, Europeans 3,107 ARID5B GATA3 influenced ALL risk Migliorini et
BFM IKZF1 and was associated with al65
worse prognosis.
CEBPE
CDKN2A
PIP4K2A (rs10828317) 1.23 1.1 to 1.3
GATA3 (rs3824662) 1.31 1.2 to 1.4
Abbreviations: AIEOP, Associazione Italiana di Ematologia Pediatrica; ALL, acute lymphoblastic leukemia; BFM, Berlin-Frankfurt-Münster; CoALL, Cooperative ALL
(study group); COG, Children’s Oncology Group; MRC, Medical Research Council; OR, odds ratio; Ph, Philadelphia chromosome; SJCRH, St Jude Children’s
Research Hospital; SNP, single nucleotide polymorphism; UK, United Kingdom; UKALL, United Kingdom Acute Lymphoblastic Leukemia (study group); UKCCS,
United Kingdom Childhood Cancer Study.
www.jco.org © 2015 by American Society of Clinical Oncology 2943
Pui et al
and the COG discovered novel ALL risk variants at the PIP4K2A- resistance,71 in vivo response to initial treatment with high-dose meth-
BMI1 locus and, for the first time, focused on multiethnic popula- otrexate,72 and inherited genome variants related to response to
tions.64 The inclusion of non-European patients in this study not only remission induction therapy.73 Indeed, both germline and somatic
improved the statistical power of detecting association signals at the genome variation can influence the effects of ALL chemotherapy,74-78
PIP4K2A variants but also revealed striking differences in the preva- which emphasizes the importance of assessing both inherited and
lence of these genetic risk variants among groups with different ances- somatic genome variation in cancer pharmacogenomics. Further-
more, genome-wide mRNA expression analyses have identified ge-
tries and their contribution to racial and ethnic differences in the
nome variation that influences the accumulation of the active
incidence of ALL. Notably, several germline susceptibility loci are
polyglutamylated metabolites of methotrexate in ALL cells after in
targeted by somatic genomic alterations in ALL blasts (IKZF1,
vivo methotrexate treatment.79,80 These studies and others have pro-
CDKN2A/CDKN2B),68 suggesting that inherited and acquired genetic vided mechanistic insights into the need for different dosages of meth-
variations should be regarded as a continuum in the development of otrexate in certain ALL subtypes (eg, higher dosage in T-ALL) and
childhood ALL. have revealed drug-specific differences in genomic determinants of de
GWASs of susceptibility to specific ALL subtypes have received novo drug resistance in childhood ALL. These findings also hold
increasing attention. In 2012, a collaborative study reported that vari- promise for developing strategies to mitigate drug resistance by target-
ants in the TP63 and PTPRJ genes were associated with the acquisition ing proteins whose overexpression or enhanced function leads to
of the ETV6-RUNX1 fusion.66 More recently, inherited variants in the resistance to conventional antileukemic agents. Ongoing genome-
GATA3 gene were associated with the development of Ph-like ALL wide interrogation of germline and somatic DNA variation (genetic
and also the increased risk of relapse in two separate studies,65,67 and epigenetic) should lead to greater insights into the mechanism of
illustrating interactions between genetic variations in the host and drug resistance and yield new treatment strategies to further enhance
those in the cancer cells and their unique contributions to pathogen- the effectiveness of ALL treatment.
esis and treatment outcomes of ALL.
GWASs have been successful in unequivocally establishing an Genomic Determinants of Drug Toxicities
inherited genetic basis for ALL susceptibility with seven risk loci Many serious toxicities of ALL therapy are relatively uncommon,
discovered thus far (Table 3). Future studies will require even more and they vary substantially in prevalence by treatment regimen. Al-
extensive intergroup collaborations to characterize the role of though genome-wide approaches have shown tremendous potential
germline genetic variations in uncommon ALL phenotypes and to for uncovering novel mechanisms and new risk factors of drug toxic-
characterize the combined effects of multiple variants acting ities, large sample sizes from collaborations are necessary to have
within the same pathway.69 adequate power to uncover underlying genomic determinants with
hazard ratios on the order of 1.5-fold to three-fold. Indeed, collabora-
Genomic Determinants of Drug Resistance tions have already identified inherited genomic variation associated with
Pharmacokinetic, pharmacodynamic, and pharmacogenomic asparaginase allergy81 and with high-dose methotrexate clearance and
studies have shown important determinants of interpatient differ- toxicity (Table 4).75,82 Other examples of inherited genomic variation that
ences in treatment response that can affect clinical outcome. Recent contribute to ALL toxicity phenotypes include the association of TPMT
technologies for interrogating inherited and acquired genome varia- variants83-87 and an NUDT15 variant88 with thiopurine-induced myelo-
tion have accelerated the discovery of genomic determinants of de suppression; CEP72 polymorphism with vincristine-related peripheral
novo drug resistance. Initially, by using genome-wide gene expression neuropathy89; CRHR1 polymorphisms and steroid-induced low bone
arrays, the expression (mRNA) of a relatively small number of genes in density, which was replicated in a pediatric asthma population90;
leukemia cells was linked to de novo sensitivity of glucocorticoids, several genes associated with osteonecrosis91,92; and methotrexate-
vincristine, daunorubicin, and L-asparaginase,70 multidrug cross- induced leukoencephalopathy.93
Table 4. Selected Examples of Genomic Determinants of Drug Toxicities Involving Multiple Collaborative Study Groups
Drug Gene Name Comments Reference
Asparaginase HLA-DRB1ⴱ07:01 HLA-DRB1ⴱ07:01-encoded protein is associated with the development of anti- Fernandez et al81
asparaginase antibody and a high frequency of asparaginase hypersensitivity,
probably through its high binding affinity for asparaginase epitopes.
Methotrexate SLCO1B1 Methotrexate clearance is associated with polymorphisms of SLCO1B1 which Treviño et al,75 Ramsey et al,77 Ramsey
encode a hepatic solute carrier organic anion transporter that mediates et al82
disposition of many medications, including methotrexate.
Mercaptopurine, TPMT Genetic polymorphisms in TPMT (thiopurine S-methyltransferase) are known to Ramsey et al,82 Lennard et al,83 Stanulla
thioguanine have a marked effect on mercaptopurine metabolism and myelosuppressive et al,84 Schmiegelow et al,85 Relling
toxicity. et al,86 Evans et al87
NUDT15 A polymorphism of NUDT15 is associated with mercaptopurine intolerance and Yang et al88
is most common in East Asians and Hispanics.
Vincristine CEP72 A polymorphism of CEP72 reduces expression of its encoded centrosomal Diouf et al89
protein 72 kD, which functions as the major microtubule-organizing center,
regulates proper bipolar spindle formation, and is associated with an
increased risk of vincristine-induced neuropathy.
2944 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Childhood ALL: Progress Through Collaboration
The underlying genomic risk factors for some adverse effects are States (eg, Therapeutic Advances in Childhood Leukemia & Lym-
likely to differ by treatment regimen. For example, asparaginase may phoma Consortium) and Europe (eg, International Study for Treat-
potentiate the osteonecrosis risk of glucocorticoids, partly via effects ment of Childhood Relapsed ALL Consortium). The VIVA-Asia
on lipid homeostasis94 and partly by affecting glucocorticoid disposi- Acute Leukemia group has recently been formed to collaborate on and
tion.95 Dosage may also play a critical role: for example, anthracycline- address the topics relevant to patients in Asia, which not only has the
induced cardiomyopathy is related to inherited variants in HAS3, but largest patient population but also has different leukemia subtypes,
only in patients who received higher cumulative doses of anthracy- environmental characteristics, population genetics, and resources.97
cline.96 By contrast, genetic risk factors for vincristine neuropathy are Historically, older adolescents and young adults had poorer treatment
apparent only at lower doses of the drug, because at higher doses, outcomes than young children and received little research attention.
almost all patients are at risk for the adverse effect.89 Because pediatric-based regimens improved outcome for this age
group,98-100 pediatric and adult oncologists have started to form con-
sortia to focus on the unique clinical, biologic, psychosocial, and
CONCLUSIONS AND FUTURE DIRECTIONS
survivorship of this age group.101 There is a great hope and expectation
that their treatment outcomes will dramatically improve in the com-
Collaborative group studies have refined the molecular classification ing years.
of ALL and have substantially improved strategies for personalized
treatment by identifying new targets for therapeutic intervention.
These collaborative studies should continue to address many unre- AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS
solved issues and questions. Next-generation sequencing studies to OF INTEREST
analyze the genome, transcriptome, and epigenome of patients will
comprehensively identify all genetic variations contributing to leuke- Disclosures provided by the authors are available with this article at
mogenesis and treatment outcome; interpreting the complex protein- www.jco.org.
protein and pathway interactions will be the challenge. Detailed
analysis of germline genetic variations will unravel the role of inherited AUTHOR CONTRIBUTIONS
polymorphisms in leukemia susceptibility and the acquisition of so-
matic genetic abnormalities. Experimental models will be developed Conception and design: Ching-Hon Pui, Allen Eng Juh Yeoh
to faithfully recapitulate the human leukemias, and novel, rationally Financial support: Ching-Hon Pui
targeted therapeutic approaches to reverse or mitigate the driver mu- Administrative support: Ching-Hon Pui, Stephen P. Hunger
tations with small molecules will become available for most patients. Provision of study materials or patients: All authors
Effective immunotherapy and cellular therapy will be developed, es- Collection and assembly of data: Ching-Hon Pui, Jun J. Yang, Lewis B.
pecially for patients with no known genetic lesions that are responsive Silverman, Kjeld Schmiegelow, Yves C.M. Benoit, Shai Izraeli
Data analysis and interpretation: Ching-Hon Pui, Jun J. Yang, Stephen
to available molecular-targeted therapy. Collaborative clinical trials P. Hunger, Martin Schrappe, Andrea Biondi, Ajay Vora, André Baruchel,
will be initiated for patients with challenging or drug-resistant leuke- Kjeld Schmiegelow, Shai Izraeli, Mary V. Relling
mia. These efforts will be extended beyond the current study groups Manuscript writing: All authors
and consortia that investigate patients residing mainly in the United Final approval of manuscript: All authors
protocol ALL-9 (1997-2004). Lancet Oncol 10:957- 10. Yeoh AE, Ariffin H, Chai EL, et al: Minimal
REFERENCES 966, 2009 residual disease-guided treatment deintensification
6. Vrooman LM, Stevenson KE, Supko JG, et for children with acute lymphoblastic leukemia:
1. Conter V, Aricò M, Basso G, et al: Long-term al: Postinduction dexamethasone and individualized Results from the Malaysia-Singapore acute lympho-
results of the Italian Association of Pediatric Hema- dosing of Escherichia Coli L-asparaginase each im- blastic leukemia 2003 study. J Clin Oncol 30:2384-
tology and Oncology (AIEOP) Studies 82, 87, 88, 91 prove outcome of children and adolescents with 2392, 2012
and 95 for childhood acute lymphoblastic leukemia. newly diagnosed acute lymphoblastic leukemia: Re- 11. Vora A, Goulden N, Mitchell C, et al: Aug-
Leukemia 24:255-264, 2010 sults from a randomized study—Dana-Farber Cancer mented post-remission therapy for a minimal resid-
2. Möricke A, Zimmermann M, Reiter A, et al: Institute ALL Consortium Protocol 00-01. J Clin ual disease-defined high-risk subgroup of children
Long-term results of five consecutive trials in child- Oncol 31:1202-1210, 2013 and young people with clinical standard-risk and
hood acute lymphoblastic leukemia performed by 7. Domenech C, Suciu S, De Moerloose B, et intermediate-risk acute lymphoblastic leukaemia
the ALL-BFM study group from 1981 to 2000. al: Dexamethasone (6 mg/m2/day) and prednisolone (UKALL 2003): A randomised controlled trial. Lancet
Leukemia 24:265-284, 2010 (60 mg/m2/day) were equally effective as induction Oncol 15:809-818, 2014
3. Escherich G, Horstmann MA, Zimmermann therapy for childhood acute lymphoblastic leukemia 12. Schmiegelow K, Forestier E, Hellebostad M,
M, et al: Cooperative study group for childhood in the EORTC CLG 58951 randomized trial. Haema- et al: Long-term results of NOPHO ALL-92 and
acute lymphoblastic leukaemia (COALL): Long-term tologica 99:1220-1227, 2014 ALL-2000 studies of childhood acute lymphoblastic
results of trials 82, 85, 89, 92 and 97. Leukemia 8. Stary J, Zimmermann M, Campbell M, et al: leukemia. Leukemia 24:345-354, 2010
24:298-308, 2010 Intensive chemotherapy for childhood acute lym- 13. Pui CH, Pei D, Campana D, et al: A revised
4. Hunger SP, Lu X, Devidas M, et al: Improved phoblastic leukemia: Results of the randomized in- definition for cure of childhood acute lymphoblastic
survival for children and adolescents with acute tercontinental trial ALL IC-BFM 2002. J Clin Oncol leukemia. Leukemia 28:2336-2343, 2014
lymphoblastic leukemia between 1990 and 2005: A 32:174-184, 2014 14. Liu HC, Yeh TC, Hou JY, et al: Triple intra-
report from the Children’s Oncology Group. J Clin 9. Yamaji K, Okamoto T, Yokota S, et al: Mini- thecal therapy alone with omission of cranial radia-
Oncol 30:1663-1669, 2012 mal residual disease-based augmented therapy in tion in children with acute lymphoblastic leukemia. J
5. Veerman AJ, Kamps WA, van den Berg H, et childhood acute lymphoblastic leukemia: A report Clin Oncol 32:1825-1829, 2014
al: Dexamethasone-based therapy for childhood from the Japanese Childhood Cancer and Leukemia 15. Downing JR, Wilson RK, Zhang J, et al: The
acute lymphoblastic leukaemia: Results of the pro- Study Group. Pediatr Blood Cancer 55:1287-1295, Pediatric Cancer Genome Project. Nat Genet 44:
spective Dutch Childhood Oncology Group (DCOG) 2010 619-622, 2012
www.jco.org © 2015 by American Society of Clinical Oncology 2945
Pui et al
16. Pui CH, Schrappe M, Masera G, et al: Ponte blastic leukemia with 11q23 rearrangements. Leu- 47. Bohnstedt C, Levinsen M, Rosthøj S, et al:
di Legno Working Group: Statement on the right of kemia 17:700-706, 2003 Physicians compliance during maintenance therapy
children with leukemia to have full access to essen- 31. Nachman JB, Heerema NA, Sather H, et al: in children with Down syndrome and acute lympho-
tial treatment and report on the Sixth International Outcome of treatment in children with hypodiploid blastic leukemia. Leukemia 27:866-870, 2013
Childhood Acute Lymphoblastic Leukemia Work- acute lymphoblastic leukemia. Blood 110:1112- 48. Buitenkamp TD, Pieters R, Gallimore NE, et
shop. Leukemia 18:1043-1053, 2004 1115, 2007 al: Outcome in children with Down’s syndrome and
17. Hunger SP, Baruchel A, Biondi A, et al: The 32. Aricò M, Valsecchi MG, Camitta B, et al: acute lymphoblastic leukemia: Role of IKZF1 dele-
thirteenth international childhood acute lymphoblas- Outcome of treatment in children with Philadelphia tions and CRLF2 aberrations. Leukemia 26:2204-
tic leukemia workshop report: La Jolla, CA, USA, chromosome-positive acute lymphoblastic leuke- 2211, 2012
December 7-9, 2011. Pediatr Blood Cancer 60:344- mia. N Engl J Med 342:998-1006, 2000 49. Mullighan CG, Collins-Underwood JR, Phil-
348, 2013 33. Aricò M, Schrappe M, Hunger SP, et al: lips LA, et al: Rearrangement of CRLF2 in
18. Schrappe M, Nachman J, Hunger S, et al: Clinical outcome of children with newly diagnosed B-progenitor- and Down syndrome-associated acute
‘Educational symposium on long-term results of Philadelphia chromosome-positive acute lympho- lymphoblastic leukemia. Nat Genet 41:1243-1246,
large prospective clinical trials for childhood acute blastic leukemia treated between 1995 and 2005. J 2009
lymphoblastic leukemia (1985-2000)’. Leukemia 24: Clin Oncol 28:4755-4761, 2010 50. Hertzberg L, Vendramini E, Ganmore I, et al:
253-254, 2010 34. Biondi A, Schrappe M, De Lorenzo P, et al: Down syndrome acute lymphoblastic leukemia, a
19. Conter V, Bartram CR, Valsecchi MG, et al: Imatinib after induction for treatment of children and highly heterogeneous disease in which aberrant
Molecular response to treatment redefines all prog- adolescents with Philadelphia-chromosome-positive expression of CRLF2 is associated with mutated
nostic factors in children and adolescents with B-cell acute lymphoblastic leukaemia (EsPhALL): A ran- JAK2: A report from the International BFM Study
precursor acute lymphoblastic leukemia: Results in domised, open-label, intergroup study. Lancet Oncol Group. Blood 115:1006-1017, 2010
3184 patients of the AIEOP-BFM ALL 2000 study. 13:936-945, 2012 51. Mullighan CG: Genomic characterization of
Blood 115:3206-3214, 2010 35. Mullighan CG, Su X, Zhang J, et al: Deletion childhood acute lymphoblastic leukemia. Semin He-
20. Schrappe M, Valsecchi MG, Bartram CR, et of IKZF1 and prognosis in acute lymphoblastic leu- matol 50:314-324, 2013
al: Late MRD response determines relapse risk kemia. N Engl J Med 360:470-480, 2009 52. Russell LJ, Capasso M, Vater I, et al: Dereg-
overall and in subsets of childhood T-cell ALL: Re- 36. Den Boer ML, van Slegtenhorst M, De Me- ulated expression of cytokine receptor gene,
sults of the AIEOP-BFM-ALL 2000 study. Blood nezes RX, et al: A subtype of childhood acute CRLF2, is involved in lymphoid transformation in
118:2077-2084, 2011 lymphoblastic leukaemia with poor treatment out- B-cell precursor acute lymphoblastic leukemia.
21. Pieters R, Schrappe M, De Lorenzo P, et al: come: A genome-wide classification study. Lancet Blood 114:2688-2698, 2009
A treatment protocol for infants younger than 1 year Oncol 10:125-134, 2009
53. Mullighan CG, Zhang J, Harvey RC, et al: JAK
with acute lymphoblastic leukaemia (Interfant-99): 37. Roberts KG, Li Y, Payne-Turner D, et al:
mutations in high-risk childhood acute lymphoblastic
An observational study and a multicentre ran- Targetable kinase-activating lesions in Ph-like acute
leukemia. Proc Natl Acad Sci U S A 106:9414-9418,
domised trial. Lancet 370:240-250, 2007 lymphoblastic leukemia. N Engl J Med 371:1005-
2009
22. Mann G, Attarbaschi A, Schrappe M, et al: Im- 1015, 2014
54. Roberts KG, Morin RD, Zhang J, et al: Ge-
proved outcome with hematopoietic stem cell transplan- 38. Coustan-Smith E, Mullighan CG, Onciu M, et
netic alterations activating kinase and cytokine re-
tation in a poor prognostic subgroup of infants with al: Early T-cell precursor leukaemia: A subtype of
ceptor signaling in high-risk acute lymphoblastic
mixed-lineage-leukemia (MLL)-rearranged acute lympho- very high-risk acute lymphoblastic leukaemia. Lan-
leukemia. Cancer Cell 22:153-166, 2012
blastic leukemia: Results from the Interfant-99 Study. cet Oncol 10:147-156, 2009
55. Weston BW, Hayden MA, Roberts KG, et al:
Blood 116:2644-2650, 2010 39. Buitenkamp TD, Izraeli S, Zimmermann M,
Tyrosine kinase inhibitor therapy induces remission
23. Childhood Acute Lymphoblastic Leukaemia et al: Acute lymphoblastic leukemia in children with
in a patient with refractory EBF1-PDGFRB-positive
Collaborative Group (CALLCG): Beneficial and harm- Down syndrome: A retrospective analysis from the
acute lymphoblastic leukemia. J Clin Oncol 31:e413-
ful effects of anthracyclines in the treatment of Ponte di Legno study group. Blood 123:70-77, 2014
e416, 2013
childhood acute lymphoblastic leukaemia: A system- 40. Schrappe M, Hunger SP, Pui CH, et al:
56. Lengline E, Beldjord K, Dombret H, et al:
atic review and meta-analysis. Br J Haematol 145: Outcomes after induction failure in childhood acute
Successful tyrosine kinase inhibitor therapy in a
376-388, 2009 lymphoblastic leukemia. N Engl J Med 366:1371-
refractory B-cell precursor acute lymphoblastic leu-
24. Eden T, Pieters R, Richards S, et al: System- 1381, 2012
atic review of the addition of vincristine plus steroid 41. Holmfeldt L, Wei L, Diaz-Flores E, et al: The kemia with EBF1-PDGFRB fusion. Haematologica
pulses in maintenance treatment for childhood genomic landscape of hypodiploid acute lympho- 98:e146-e148, 2013
acute lymphoblastic leukaemia: An individual patient blastic leukemia. Nat Genet 45:242-252, 2013 57. Homminga I, Pieters R, Langerak AW, et al:
data meta-analysis involving 5,659 children. Br J 42. Schultz KR, Carroll A, Heerema NA, et al: Integrated transcript and genome analyses reveal
Haematol 149:722-733, 2010 Long-term follow-up of imatinib in pediatric Philadel- NKX2-1 and MEF2C as potential oncogenes in T cell
25. Escherich G, Richards S, Stork LC, et al: phia chromosome-positive acute lymphoblastic leu- acute lymphoblastic leukemia. Cancer Cell 19:484-
Meta-analysis of randomised trials comparing thio- kemia: Children’s Oncology Group study AALL0031. 497, 2011
purines in childhood acute lymphoblastic leukaemia. Leukemia 28:1467-1471, 2014 58. Zhang J, Ding L, Holmfeldt L, et al: The
Leukemia 25:953-959, 2011 43. Zwaan CM, Rizzari C, Mechinaud F, et al: genetic basis of early T-cell precursor acute lympho-
26. Richards S, Pui CH, Gayon P, et al: System- Dasatinib in children and adolescents with relapsed blastic leukaemia. Nature 481:157-163, 2012
atic review and meta-analysis of randomized trials of or refractory leukemia: Results of the CA180-018 59. Treanor LM, Zhou S, Janke L, et al:
central nervous system directed therapy for child- phase I dose-escalation study of the Innovative Interleukin-7 receptor mutants initiate early T cell
hood acute lymphoblastic leukemia. Pediatr Blood Therapies for Children with Cancer Consortium. J precursor leukemia in murine thymocyte progeni-
Cancer 60:185-195, 2013 Clin Oncol 31:2460-2468, 2013 tors with multipotent potential. J Exp Med 211:701-
27. Pieters R, Hunger SP, Boos J, et al: 44. van der Veer A, Waanders E, Pieters R, et al: 713, 2014
L-asparaginase treatment in acute lymphoblastic Independent prognostic value of BCR-ABL1-like sig- 60. Shah S, Schrader KA, Waanders E, et al: A
leukemia: A focus on Erwinia asparaginase. Cancer nature and IKZF1 deletion, but not high CRLF2 recurrent germline PAX5 mutation confers suscep-
117:238-249, 2011 expression, in children with B-cell precursor ALL. tibility to pre-B cell acute lymphoblastic leukemia.
28. Tong WH, Pieters R, Kaspers GJ, et al: A Blood 122:2622-2629, 2013 Nat Genet 45:1226-1231, 2013
prospective study on drug monitoring of PEGaspara- 45. Roberts KG, Pei D, Campana D, et al: Out- 61. Treviño LR, Yang W, French D, et al: Germ-
ginase and Erwinia asparaginase and asparaginase come of children with BCR-ABL1–like acute lympho- line genomic variants associated with childhood
antibodies in pediatric acute lymphoblastic leuke- blastic leukemia treated with risk-directed therapy acute lymphoblastic leukemia. Nat Genet 41:1001-
mia. Blood 123:2026-2033, 2014 based on the levels of minimal residual disease. J 1005, 2009
29. Pui CH, Gaynon PS, Boyett JM, et al: Out- Clin Oncol 32:3012-3020, 2014 62. Papaemmanuil E, Hosking FJ, Vijayakrishnan
come of treatment in childhood acute lymphoblastic 46. Patrick K, Wade R, Goulden N, et al: Out- J, et al: Loci on 7p12.2, 10q21.2 and 14q11.2 are
leukaemia with rearrangements of the 11q23 chro- come for children and young people with early T-cell associated with risk of childhood acute lymphoblas-
mosomal region. Lancet 359:1909-1915, 2002 precursor acute lymphoblastic leukaemia treated on tic leukemia. Nat Genet 41:1006-1010, 2009
30. Pui CH, Chessells JM, Camitta B, et al: a contemporary protocol, UKALL 2003. Br J Haema- 63. Sherborne AL, Hosking FJ, Prasad RB, et al:
Clinical heterogeneity in childhood acute lympho- tol 166:421-424, 2014 Variation in CDKN2A at 9p21.3 influences childhood
2946 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Childhood ALL: Progress Through Collaboration
acute lymphoblastic leukemia risk. Nat Genet 42: stability cause DNA mismatch repair deficiency and related peripheral neuropathy in children with acute
492-494, 2010 drug resistance in human leukemia cells. Nat Med lymphoblastic leukemia. JAMA 313:815-823, 2015
64. Xu H, Yang W, Perez-Andreu V, et al: Novel 17:1298-1303, 2011 90. Jones TS, Kaste SC, Liu W, et al: CRHR1
susceptibility variants at 10p12.31-12.2 for child- 77. Ramsey LB, Bruun GH, Yang W, et al: Rare polymorphisms predict bone density in survivors of
hood acute lymphoblastic leukemia in ethnically versus common variants in pharmacogenetics: acute lymphoblastic leukemia. J Clin Oncol 26:3031-
diverse populations. J Natl Cancer Inst 105:733-742, SLCO1B1 variation and methotrexate disposition. 3037, 2008
2013 Genome Res 22:1-8, 2012 91. Relling MV, Yang W, Das S, et al: Pharmaco-
65. Migliorini G, Fiege B, Hosking FJ, et al: 78. Gregers J, Christensen IJ, Dalhoff K, et al: genetic risk factors for osteonecrosis of the hip
Variation at 10p12.2 and 10p14 influences risk of The association of reduced folate carrier 80G⬎A among children with leukemia. J Clin Oncol 22:
childhood B-cell acute lymphoblastic leukemia and polymorphism to outcome in childhood acute lym- 3930-3936, 2004
phenotype. Blood 122:3298-3307, 2013 phoblastic leukemia interacts with chromosome 21 92. French D, Hamilton LH, Mattano LA Jr, et al:
66. Ellinghaus E, Stanulla M, Richter G, et al: copy number. Blood 115:4671-4677, 2010 A PAI-1 (SERPINE1) polymorphism predicts osteo-
Identification of germline susceptibility loci in ETV6- 79. Kager L, Cheok M, Yang W, et al: Folate necrosis in children with acute lymphoblastic leuke-
RUNX1-rearranged childhood acute lymphoblastic pathway gene expression differs in subtypes of mia: A report from the Children’s Oncology Group.
leukemia. Leukemia 26:902-909, 2012 acute lymphoblastic leukemia and influences meth- Blood 111:4496-4499, 2008
67. Perez-Andreu V, Roberts KG, Harvey RC, et otrexate pharmacodynamics. J Clin Invest 115:110- 93. Bhojwani D, Sabin ND, Pei D, et al:
al: Inherited GATA3 variants are associated with 117, 2005 Methotrexate-induced neurotoxicity and leukoen-
Ph-like childhood acute lymphoblastic leukemia and 80. Belkov VM, Krynetski EY, Schuetz JD, et al: cephalopathy in childhood acute lymphoblastic leu-
risk of relapse. Nat Genet 45:1494-1498, 2013 Reduced folate carrier expression in acute lympho- kemia. J Clin Oncol 32:949-959, 2014
68. Mullighan CG, Goorha S, Radtke I, et al: blastic leukemia: A mechanism for ploidy but not 94. Dumitrescu L, Brown-Gentry K, Goodloe R,
Genome-wide analysis of genetic alterations in lineage differences in methotrexate accumulation. et al: Evidence for age as a modifier of genetic
acute lymphoblastic leukaemia. Nature 446:758- Blood 93:1643-1650, 1999
associations for lipid levels. Ann Hum Genet 75:589-
764, 2007 81. Fernandez CA, Smith C, Yang W, et al:
597, 2011
69. Wesołowska-Andersen A, Borst L, Dalgaard HLA-DRB1*07:01 is associated with a higher risk of
95. Kawedia JD, Liu C, Pei D, et al: Dexametha-
MD, et al: Genomic profiling of thousands of candi- asparaginase allergies. Blood 124:1266-1276, 2014
sone exposure and asparaginase antibodies affect
date polymorphisms predicts risk of relapse in 778 82. Ramsey LB, Panetta JC, Smith C, et al:
relapse risk in acute lymphoblastic leukemia. Blood
Danish and German childhood acute lymphoblastic Genome-wide study of methotrexate clearance rep-
119:1658-1664, 2012
leukemia patients. Leukemia 29:297-303, 2015 licates SLCO1B1. Blood 121:898-904, 2013
96. Wang X, Liu W, Sun CL, et al: Hyaluronan
70. Holleman A, Cheok MH, den Boer ML, et al: 83. Lennard L, Lilleyman JS, Van Loon J, et al:
synthase 3 variant and anthracycline-related cardio-
Gene expression patterns in drug resistance acute Genetic variation in response to 6-mercaptopurine
myopathy: A report from the Children’s Oncology
lymphoblastic leukemia and response to treatment. for childhood acute lymphoblastic leukaemia. Lancet
Group. J Clin Oncol 32:647-653, 2014
N Engl J Med 351:533-542, 2004 336:225-229, 1990
97. Yeoh AE, Tan D, Li CK, et al: Management of
71. Lugthart S, Cheok MH, den Boer ML, et al: 84. Stanulla M, Schaeffeler E, Flohr T, et al:
adult and paediatric acute lymphoblastic leukaemia
Identification of genes associated with chemother- Thiopurine methyltransferase (TPMT) genotype and
apy crossresistance and treatment response in early treatment response to mercaptopurine in child- in Asia: Resource-stratified guidelines from the
childhood acute lymphoblastic leukemia. Cancer hood acute lymphoblastic leukemia. JAMA 293: Asian Oncology Summit 2013. Lancet Oncol 14:
Cell 7:375-386, 2005 1485-1489, 2005 e508-e523, 2013
72. Sorich M, Pottier N, Pei D, et al: In vivo 85. Schmiegelow K, Forestier E, Kristinsson J, et 98. Stock W, La M, Sanford B, et al: What
response to methotrexate forecasts outcome of al: Thiopurine methyltransferase activity is related to determines the outcomes for adolescents and
acute lymphoblastic leukemia and has a distinct the risk of relapse of childhood acute lymphoblastic young adults with acute lymphoblastic leukemia
gene expression profile. PLoS Med 5:e83, 2008 leukemia: Results from the NOPHO ALL-92 study. treated on cooperative group protocols? A compar-
73. Yang JJ, Cheng C, Yang W, et al: Genome- Leukemia 23:557-564, 2009 ison of Children’s Cancer Group and Cancer and
wide interrogation of germline genetic variation as- 86. Relling MV, Hancock ML, Rivera GK, et al: Leukemia Group B studies. Blood 112:1646-1654,
sociated with treatment response in childhood Mercaptopurine therapy intolerance and heterozy- 2008
acute lymphoblastic leukemia. JAMA 301:393-403, gosity at the thiopurine S-methyltransferase gene 99. Boissel N, Auclerc MF, Lhéritier V, et al:
2009 locus. J Natl Cancer Inst 91:2001-2008, 1999 Should adolescents with acute lymphoblastic leuke-
74. Cheng Q, Yang W, Raimondi SC, et al: Karyo- 87. Evans WE, Hon YY, Bomgaars L, et al: mia be treated as old children or young adults?
typic abnormalities create discordance of germline Preponderance of thiopurine S-methyltransferase Comparison of the French FRALLE-93 and LALA-94
genotype and cancer cell phenotypes. Nat Genet deficiency and heterozygosity among patients intol- trials. J Clin Oncol 21:774-780, 2003
37:878-882, 2005 erant to mercaptopurine or azathioprine. J Clin On- 100. Pui CH, Pei D, Campana D, et al: Improved
75. Treviño LR, Shimasaki N, Yang W, et al: col 19:2293-2301, 2001 prognosis for older adolescents with acute lympho-
Germline genetic variation in an organic anion trans- 88. Yang JJ, Landier W, Yang W, et al: Inherited blastic leukemia. J Clin Oncol 29:386-391, 2011
porter polypeptide associated with methotrexate NUDT15 variant is a genetic determinant of mercap- 101. Toft N, Birgens H, Abrahamsson J, et al: Risk
pharmacokinetics and clinical effects. J Clin Oncol topurine intolerance in children with acute lympho- group assignment differs for children and adults
27:5972-5978, 2009 blastic leukemia. J Clin Oncol 33:1235-1242, 2015 1-45 yr with acute lymphoblastic leukemia treated
76. Diouf B, Cheng Q, Krynetskaia NF, et al: 89. Diouf B, Crews KR, Lew G, et al: Association by the NOPHO ALL-2008 protocol. Eur J Haematol
Somatic deletions of genes regulating MSH2 protein of an inherited genetic variant with vincristine- 90:404-412, 2013
Affiliations
Ching-Hon Pui, Jun J. Yang, James R. Downing, Williams E. Evans, Mary V. Relling, and Charles G. Mullighan, St Jude Children’s
Research Hospital and the University of Tennessee Health Science Center, Memphis, TN; Stephen P. Hunger, University of Colorado School
of Medicine and the University of Colorado Cancer Center and Children’s Hospital Colorado, Aurora, CO; Rob Pieters, Princess Máxima
Center for Pediatric Oncology, Utrecht, the Netherlands; Martin Schrappe, University Medical Center Schleswig-Holstein, Christian-
Albrechts-University, Kiel; Gabriele Escherich, Clinic of Pediatric Hematology and Oncology, University Medical Center Hamburg
Eppendorf, Hamburg, Germany; Andrea Biondi, Clinica Pediatrica and Centro Ricerca Tettamanti, Università di Milano-Bicocca, Monza,
Italy; Ajay Vora, Children’s Cancer Group, School of Cancer, Manchester Academic Health Sciences Centre, University of Manchester,
Manchester, United Kingdom; André Baruchel, Hôpital Robert Debré and University of Paris Diderot, Paris, France; Lewis B. Silverman,
Dana-Farber Cancer Institute and Boston Children’s Hospital, Boston, MA; Kjeld Schmiegelow, Institute of Clinical Medicine, University of
Copenhagen and Juliane Marie Centre, the University Hospital Rigshospitalet, Copenhagen, Denmark; Keizo Horibe, Nagoya Medical
Center, Clinical Research Center, Nagoya, Japan; Yves C.M. Benoit, Universiteit Gent, Gent, Belgium; Shai Izraeli, Chaim Sheba Medical
www.jco.org © 2015 by American Society of Clinical Oncology 2947
Pui et al
Center and Sackler Medical School, Tel Aviv University, Tel Aviv, Israel; Allen Eng Juh Yeoh, Yong Loo Lin School of Medicine and Cancer
Science Institute, National University of Singapore, and Viva-University Children’s Cancer Centre, National University Hospital, Singapore;
and Der-Cherng Liang, Mackay Memorial Hospital, Taipei, Taiwan.
■ ■ ■
Get the Managing the Cost of Cancer Care
Booklets for Your Practice
Do your patients have financial questions about cancer care? Cancer.Net’s
Managing the Cost of Cancer Care booklet provides tools and
resources that can help your patients answer these questions and
plan for costs before, during, and after treatment. Order copies of the booklet for your
patients through the ASCO University Bookstore at www.cancer.net/estore.
ASCO members receive a 20% discount. The booklet is also available as a downloadable
PDF in English and Spanish at cancer.net/managingcostofcare.
2948 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Childhood ALL: Progress Through Collaboration
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Childhood Acute Lymphoblastic Leukemia: Progress Through Collaboration
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are
self-held unless noted. I ⫽ Immediate Family Member, Inst ⫽ My Institution. Relationships may not relate to the subject matter of this manuscript. For more
information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or jco.ascopubs.org/site/ifc.
Ching-Hon Pui Lewis B. Silverman
No relationship to disclose Consulting or Advisory Role: Epizyme, Seattle Genetics
Research Funding: Sigma Tau Pharmaceuticals
Jun J. Yang
No relationship to disclose Kjeld Schmiegelow
No relationship to disclose
Stephen P. Hunger
Stock or Other Ownership: Express Scripts, Amgen, Merck (I), Amgen Gabriele Escherich
(I), Pfizer (I) No relationship to disclose
Honoraria: Jazz Pharmaceuticals, Sigma Tau Pharmaceuticals Keizo Horibe
Patents, Royalties, Other Intellectual Property: I am a co-inventor on a No relationship to disclose
US patent #8,568,974 B2: Identification of novel subgroups of high-risk
pediatric precursor-B acute lymphoblastic leukemia, outcome Yves C.M. Benoit
correlations and diagnostic and therapeutic methods related to same. It No relationship to disclose
has not been licensed and there is no income Shai Izraeli
Travel, Accommodations, Expenses: Amgen Consulting or Advisory Role: Novartis
Research Funding: Pfizer
Rob Pieters
Patents, Royalties, Other Intellectual Property: US patent 8,841,266.
No relationship to disclose
Pharmacological composition and method for regulating abnormal
Martin Schrappe cellular proliferation
Consulting or Advisory Role: Novartis Allen Eng Juh Yeoh
Research Funding: SigmaTau Pharmaceuticals (Inst), Jazz Speakers’ Bureau: Sanofi
Pharmaceuticals (Inst)
Travel, Accommodations, Expenses: Medac Pharma Der-Cherng Liang
No relationship to disclose
Andrea Biondi
No relationship to disclose James R. Downing
No relationship to disclose
Ajay Vora
Consulting or Advisory Role: Jazz Pharmaceuticals, Novartis William E. Evans
No relationship to disclose
André Baruchel
Honoraria: Sigma Tau Pharmaceuticals Mary V. Relling
Patents, Royalties, Other Intellectual Property: Prometheus
Consulting or Advisory Role: Jazz Pharmaceuticals, Novartis, Seattle
Laboratories, royalties from licensing TPMT genotyping
Genetics, Pfizer, Servier
Travel, Accommodations, Expenses: ARIAD Pharmaceuticals, Jazz Charles G. Mullighan
Pharmaceuticals No relationship to disclose
www.jco.org © 2015 by American Society of Clinical Oncology
You might also like
- Treatmentof Pediatric Acute Lymphoblastic Leukemiaand Recent AdvancesDocument17 pagesTreatmentof Pediatric Acute Lymphoblastic Leukemiaand Recent AdvancesRizkaNo ratings yet
- New Approaches To Treating Challenging Subtypes of ALL in AYADocument19 pagesNew Approaches To Treating Challenging Subtypes of ALL in AYAKarol CriscuoloNo ratings yet
- Mcneer2010 Optimal Use Steroids in Pediatric ALL No Easy AnswersDocument15 pagesMcneer2010 Optimal Use Steroids in Pediatric ALL No Easy AnswersAmairani MorenoNo ratings yet
- Supportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachFrom EverandSupportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachJames H. FeusnerNo ratings yet
- Medical and Pediatric Oncology Volume 34 Issue 2 2000 (Doi 10.1002 - (Sici) 1096-911x (200002) 34!2!92 - Aid-Mpo3 - 3.0.co 2-q) Bennett, Charles L. Stinson, Tammy J. Lane, David AmyloDocument5 pagesMedical and Pediatric Oncology Volume 34 Issue 2 2000 (Doi 10.1002 - (Sici) 1096-911x (200002) 34!2!92 - Aid-Mpo3 - 3.0.co 2-q) Bennett, Charles L. Stinson, Tammy J. Lane, David AmyloNisha RehmanNo ratings yet
- British Journal Hematology AML TrialDocument10 pagesBritish Journal Hematology AML TrialRahul B SNo ratings yet
- Bab 2Document16 pagesBab 2jihan febriyantiNo ratings yet
- CANCER UPDATE Clinical Stem Cell Document - Alex Mou & Ryan TangDocument7 pagesCANCER UPDATE Clinical Stem Cell Document - Alex Mou & Ryan Tangalexmou2008No ratings yet
- Sciencedirect: Original ResearchDocument8 pagesSciencedirect: Original ResearchThiamNo ratings yet
- The Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationDocument21 pagesThe Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationGarsa GarnolNo ratings yet
- Critical Reviews in Oncology / HematologyDocument14 pagesCritical Reviews in Oncology / HematologyMIGUEL MORENONo ratings yet
- Asco GCSF 2015Document16 pagesAsco GCSF 2015Alvy SyukrieNo ratings yet
- Repetto 2003Document9 pagesRepetto 2003majedNo ratings yet
- Gene Therapy Clinical Trials Worldwide To 2017 An UpdateDocument16 pagesGene Therapy Clinical Trials Worldwide To 2017 An UpdateLeonardo Sandi SalazarNo ratings yet
- A Systematic Literature Review of The Efficacy, Effectiveness, and Safety of FilgrastimDocument14 pagesA Systematic Literature Review of The Efficacy, Effectiveness, and Safety of FilgrastimNo NameNo ratings yet
- Regimen Calgb 8811Document14 pagesRegimen Calgb 8811ricardo_cheNo ratings yet
- 1 s2.0 S0305737217300531 MainDocument11 pages1 s2.0 S0305737217300531 MaindadupipaNo ratings yet
- Efficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC StudyDocument1 pageEfficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC Studyjuloc34No ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Research PaperDocument14 pagesResearch PaperlilisNo ratings yet
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocument9 pagesYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliNo ratings yet
- Combination TACE Plus Sorafebin, Systematic ReviewDocument8 pagesCombination TACE Plus Sorafebin, Systematic ReviewMuhammad Yusuf HanifNo ratings yet
- EVIDoa 2200015Document11 pagesEVIDoa 2200015Gustavo BraccoNo ratings yet
- Guidelines For The Diagnosis and Management of Hirschsprung-Associated EnterocolitisDocument5 pagesGuidelines For The Diagnosis and Management of Hirschsprung-Associated EnterocolitisNasrudin EfendiNo ratings yet
- Fphar 13 970978Document7 pagesFphar 13 970978Claudiu PopescuNo ratings yet
- Ournal of Linical Ncology: PurposeDocument7 pagesOurnal of Linical Ncology: PurposeIvor Wiguna Hartanto WilopoNo ratings yet
- Original Research PaperDocument4 pagesOriginal Research PaperDr SrigopalNo ratings yet
- Prevalensi Dan Faktor AsosiasiDocument11 pagesPrevalensi Dan Faktor Asosiasisahama2508No ratings yet
- S1359634912X00028 S1359634912700253 MainDocument7 pagesS1359634912X00028 S1359634912700253 MainindracuangNo ratings yet
- Sickle Cell Literature ReviewDocument8 pagesSickle Cell Literature Reviewafdtnybjp100% (1)
- Successful Management of Granulocytic Sarcoma With Co - 2016 - Pediatric HematolDocument2 pagesSuccessful Management of Granulocytic Sarcoma With Co - 2016 - Pediatric HematolHawin NurdianaNo ratings yet
- Precision Medicine in Pediatric Oncology: ReviewDocument8 pagesPrecision Medicine in Pediatric Oncology: ReviewCiocan AlexandraNo ratings yet
- VasculitisDocument12 pagesVasculitisMaite OrellanaNo ratings yet
- Pharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeDocument3 pagesPharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeiajpsNo ratings yet
- Gerd CPG PDFDocument17 pagesGerd CPG PDFJamie SebastianNo ratings yet
- ST Gallen 1988Document5 pagesST Gallen 1988Nicola CrestiNo ratings yet
- Angiogenesis: What We Know, What We Do Not Understand Yet, and What We Have To DoDocument2 pagesAngiogenesis: What We Know, What We Do Not Understand Yet, and What We Have To DoAnca Maria CimpeanNo ratings yet
- MM GuidelineDocument40 pagesMM GuidelineANDREANo ratings yet
- A Multicentre, Randomised, Double Blind, Phase IIDocument11 pagesA Multicentre, Randomised, Double Blind, Phase IIveaceslav coscodanNo ratings yet
- Dialyzer Membrane Permeability and Survi PDFDocument7 pagesDialyzer Membrane Permeability and Survi PDFNurul SaufikaNo ratings yet
- The Diagnostic Criteria For Chronic EndometritisDocument7 pagesThe Diagnostic Criteria For Chronic EndometritisyuriescaidaNo ratings yet
- Comparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis MediaDocument8 pagesComparison of Amoxicillin/Clavulanic Acid High Dose With Cef Dinir in The Treatment of Acute Otitis Mediaenggainget8663No ratings yet
- Healthcare Cost and Utilization in Nonalcoholic Fatty Liver Disease: Real World Data From A Large US Claims DatabaseDocument27 pagesHealthcare Cost and Utilization in Nonalcoholic Fatty Liver Disease: Real World Data From A Large US Claims DatabaseAnonymous Xx62oL0diMNo ratings yet
- LeprosyDocument20 pagesLeprosyHafiz Sulistio UtomoNo ratings yet
- Simtomax: A New Screening Tool For Coeliac Disease: Linda MizenDocument6 pagesSimtomax: A New Screening Tool For Coeliac Disease: Linda MizenmarcosNo ratings yet
- The Association Between Iron Deficiency and Otitis Media With EffusionDocument4 pagesThe Association Between Iron Deficiency and Otitis Media With EffusionFelicia FloraNo ratings yet
- DCE and DW-MRI Monitoring of Vascular Disruption Following VEGF-Trap Treatment of A Rat Glioma ModelDocument22 pagesDCE and DW-MRI Monitoring of Vascular Disruption Following VEGF-Trap Treatment of A Rat Glioma ModelDong DongNo ratings yet
- 2022 JastreboffDocument12 pages2022 JastreboffSinityNo ratings yet
- 10 Carcinomatoza PeritonealaDocument9 pages10 Carcinomatoza PeritonealaGabriela MilitaruNo ratings yet
- Impact of Estrogen Type On Cardiovascular Safety of Combined OralDocument12 pagesImpact of Estrogen Type On Cardiovascular Safety of Combined OralMary SuescaNo ratings yet
- Recommendations For Reporting Results of Diagnostic Genetic Testing (Biochemical, Cytogenetic and Molecular Genetic)Document11 pagesRecommendations For Reporting Results of Diagnostic Genetic Testing (Biochemical, Cytogenetic and Molecular Genetic)Fearless AngelNo ratings yet
- Nejmoa 1917246Document12 pagesNejmoa 1917246AmitShettyNo ratings yet
- Thematic Abstract Review: Systemic Factors Affecting Implant Survival?Document3 pagesThematic Abstract Review: Systemic Factors Affecting Implant Survival?Natalia Camila Rodríguez LatorreNo ratings yet
- Clinical Trials For Pediatric Oncology PatientsDocument6 pagesClinical Trials For Pediatric Oncology Patientsapi-284599584No ratings yet
- Translating Best Evidence Into Best CareDocument4 pagesTranslating Best Evidence Into Best CareJorge Vivanco RiosNo ratings yet
- Integrated Onco-Palliative Care Associated WithDocument6 pagesIntegrated Onco-Palliative Care Associated WithKayoNo ratings yet
- Chronic Lymphocytic Leukemia in Young (Comprehensive Analysis of Prognostic Factors and OutcomesDocument40 pagesChronic Lymphocytic Leukemia in Young (Comprehensive Analysis of Prognostic Factors and OutcomesSanti Ayu SNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityWarun KumarNo ratings yet
- Debiopharm - Company-ProfileDocument42 pagesDebiopharm - Company-ProfileCarmen AdlerNo ratings yet
- Management of Spa Pools Controlling The Risk Oof Infections Part 2Document88 pagesManagement of Spa Pools Controlling The Risk Oof Infections Part 2VicktorNo ratings yet
- Notre Dame MODULE 3Document10 pagesNotre Dame MODULE 3Alpha-z PrinNo ratings yet
- Excerpt From A Journal of The Plague YearDocument3 pagesExcerpt From A Journal of The Plague YearErnez LaurenceNo ratings yet
- November 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Document20 pagesNovember 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Chris SoksNo ratings yet
- Major Insect Pest Management of Sugarcane CropDocument11 pagesMajor Insect Pest Management of Sugarcane CropAbdul GhaffarNo ratings yet
- Non-Communicable Diseases - Lifestyle Related Diseases: Wilma N. Beralde, RM, RN, ManDocument53 pagesNon-Communicable Diseases - Lifestyle Related Diseases: Wilma N. Beralde, RM, RN, ManNaddy RetxedNo ratings yet
- Done 3Document51 pagesDone 3ali edreesNo ratings yet
- Argumentative EssaysDocument40 pagesArgumentative Essaysphamvi44552002No ratings yet
- Pentose Phosphate Pathway: M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDocument22 pagesPentose Phosphate Pathway: M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDr. M. Prasad NaiduNo ratings yet
- New Singulair MontelukastDocument1 pageNew Singulair MontelukastCassie100% (2)
- ASRS 5 EnglishDocument3 pagesASRS 5 EnglishJavier Cotobal100% (1)
- Renr Week 7th 2017 Questions SheetDocument21 pagesRenr Week 7th 2017 Questions SheetSasha UterNo ratings yet
- Antimicrobial Activity of Citrus SinensisDocument44 pagesAntimicrobial Activity of Citrus SinensisherrNo ratings yet
- Model State Medical Marijuana Bill PDFDocument26 pagesModel State Medical Marijuana Bill PDFJoseph PreisterNo ratings yet
- Joining Instructions Indian Military Academy (IMA) Dehradun - 28-Nov-2011 - IMAJOININGINSTRUCTIONSDocument29 pagesJoining Instructions Indian Military Academy (IMA) Dehradun - 28-Nov-2011 - IMAJOININGINSTRUCTIONSChander JoonNo ratings yet
- NURS FPX 6614 Assessment 1 Defining A Gap in PracticeDocument6 pagesNURS FPX 6614 Assessment 1 Defining A Gap in Practicezadem5266No ratings yet
- Ocd EngDocument8 pagesOcd Engritagema100% (1)
- Forte-ASD BLDG Sci FocusDocument12 pagesForte-ASD BLDG Sci FocusElena Cătălina IktimurNo ratings yet
- Residual Ridge Resorpion With ManagementDocument47 pagesResidual Ridge Resorpion With ManagementAbhishek Gupta0% (1)
- Chapter 024wong S Essentials of Pediatrics Test BankDocument21 pagesChapter 024wong S Essentials of Pediatrics Test BankLLLJJJNo ratings yet
- Marketing AnalysisDocument6 pagesMarketing AnalysisSwagato SarkarNo ratings yet
- KAQdTHuFSWKATOwEayAf SFE VineetSharma PDFDocument326 pagesKAQdTHuFSWKATOwEayAf SFE VineetSharma PDFsailushaNo ratings yet
- Human Immunodeficiency Virus: Presented by Rughoobur Chitra Group 2 (A) Faculty of Foreign StudentsDocument51 pagesHuman Immunodeficiency Virus: Presented by Rughoobur Chitra Group 2 (A) Faculty of Foreign StudentskrughooburNo ratings yet
- Chapter 3 Lesson 3 ProtozoaDocument17 pagesChapter 3 Lesson 3 ProtozoaKreizel FajaNo ratings yet
- JKLDocument26 pagesJKLDragana ObradovićNo ratings yet
- HysterectomyDocument25 pagesHysterectomyCreighton A. BayonganNo ratings yet
- Beddis2014 Management of Deep Overbite PDFDocument7 pagesBeddis2014 Management of Deep Overbite PDFnithya_sendhilNo ratings yet
- HYPERTENSION-WPS OfficeDocument4 pagesHYPERTENSION-WPS OfficeAMOS MELINo ratings yet
- 5 E Coli in UTIDocument7 pages5 E Coli in UTIGhadah AlyousifNo ratings yet