You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ITE Crash Course - CardiologyDocument260 pagesITE Crash Course - CardiologyDre2323No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mastering Electocardiograms - Honda-2Document3 pagesMastering Electocardiograms - Honda-2Christian MacielNo ratings yet
- AP WindowDocument13 pagesAP WindowHugo GonzálezNo ratings yet
- Acute Arterial OcclusionDocument44 pagesAcute Arterial OcclusionAlbertus Maria Henry SantosoNo ratings yet
- Tabark Radhi - Benign Breast NeoplasmDocument19 pagesTabark Radhi - Benign Breast NeoplasmAhmed AliNo ratings yet
- Tabark Radhi - Uterine LeiomyomaDocument7 pagesTabark Radhi - Uterine LeiomyomaAhmed AliNo ratings yet
- Ahmed Ali - CKDDocument20 pagesAhmed Ali - CKDAhmed AliNo ratings yet
- Ahmed Ali - Epidemiology and Diagnosis of ALLDocument10 pagesAhmed Ali - Epidemiology and Diagnosis of ALLAhmed AliNo ratings yet
- Ahmed Ali - AdenomyosisDocument6 pagesAhmed Ali - AdenomyosisAhmed AliNo ratings yet
- Anatomy Myocardial InfarctionDocument5 pagesAnatomy Myocardial InfarctionLyka Milo AvilaNo ratings yet
- 2 - Holter ECG - TLC5000 Dynamic ECG SystemDocument3 pages2 - Holter ECG - TLC5000 Dynamic ECG SystemChristian Donfack fogang100% (1)
- ECG Fast and Easy chp12 PDFDocument40 pagesECG Fast and Easy chp12 PDFkikyfauziaNo ratings yet
- Carson LiberalvsRestrictiveTransfusionforSymptomaticCAD AmHeartJ 2013 PDFDocument9 pagesCarson LiberalvsRestrictiveTransfusionforSymptomaticCAD AmHeartJ 2013 PDFDio AlexanderNo ratings yet
- Ekg BasicDocument24 pagesEkg BasicGhica CostinNo ratings yet
- Valvular Heart DiseasesDocument29 pagesValvular Heart Diseasesbpt2No ratings yet
- Intraoperative Cardiac ArrestDocument19 pagesIntraoperative Cardiac ArrestMark Andrew CruzNo ratings yet
- Arrhythmia Diagnosis and ManagementDocument44 pagesArrhythmia Diagnosis and ManagementanwarNo ratings yet
- Program at A Glance 30th Asmiha, Isci, Ina-Chd - 12oct2021Document13 pagesProgram at A Glance 30th Asmiha, Isci, Ina-Chd - 12oct2021Rizki Anindita MtdNo ratings yet
- Jugular Venous Pressure: It's Easier Than It LooksDocument25 pagesJugular Venous Pressure: It's Easier Than It LooksManggarsari SdwqNo ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
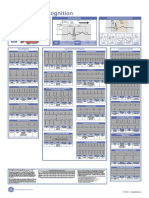
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFMiko RamosoNo ratings yet
- Go Red For Women PresentationDocument31 pagesGo Red For Women PresentationadithiNo ratings yet
- 6 Minute Walk TestDocument12 pages6 Minute Walk TestAnanth NagarajNo ratings yet
- Ton Mitral Valve ReplacementDocument3 pagesTon Mitral Valve ReplacementSony TonNo ratings yet
- Clinical Demonstration: Topic: Electrocardiogram (ECG)Document24 pagesClinical Demonstration: Topic: Electrocardiogram (ECG)soniya josephNo ratings yet
- Hipertensi: Winny Mutia FranciskaDocument4 pagesHipertensi: Winny Mutia FranciskaFranciska MuthiaNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Bradycardia and TachycardiaDocument50 pagesBradycardia and Tachycardialiu_owen17No ratings yet
- CHD Managemen Withot Surgery Cansy JHC (Prof. Mul) PDFDocument39 pagesCHD Managemen Withot Surgery Cansy JHC (Prof. Mul) PDFFery NurjayantoNo ratings yet
- CardiomyopathyDocument21 pagesCardiomyopathyapi-489918644No ratings yet
- CH 18 Casestudy With Worksheet-2Document2 pagesCH 18 Casestudy With Worksheet-2Yanitza Yanez0% (1)
- Daftar Pustaka ImaDocument2 pagesDaftar Pustaka ImaDesrina PungkyNo ratings yet
- Congestive Heart FailureDocument29 pagesCongestive Heart FailureAbby Ang100% (3)
- Myocardial Infarction: Presentation by 1605-Abubakkar Raheel 1622 - Haider Ali 1606 - Ahmed Arsalan 1611 - Amaila AnamDocument38 pagesMyocardial Infarction: Presentation by 1605-Abubakkar Raheel 1622 - Haider Ali 1606 - Ahmed Arsalan 1611 - Amaila Anamfurr singhNo ratings yet
- LeukemiaDocument5 pagesLeukemiaNourie BerawiNo ratings yet