You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Surgical Nursing 7th Edition Ignatavicius Test BankDocument9 pagesMedical Surgical Nursing 7th Edition Ignatavicius Test Bankqocax0% (1)
- The Swoosh English Guide To OET WritingDocument20 pagesThe Swoosh English Guide To OET WritingHosiah-Jen Mateo71% (7)
- MRKH Sundrome PPTDocument37 pagesMRKH Sundrome PPTleenarobin100% (2)
- Ophthalmology: NEET PG 2020 QuestionsDocument17 pagesOphthalmology: NEET PG 2020 QuestionsAnmol KudalNo ratings yet
- AUGMENTIN Tablets: What Is in This Leaflet?Document4 pagesAUGMENTIN Tablets: What Is in This Leaflet?Anmol KudalNo ratings yet
- Chronic Functional Abdominal Pain: Pathophysiology - Understanding Why People Get CfapDocument3 pagesChronic Functional Abdominal Pain: Pathophysiology - Understanding Why People Get CfapAnmol KudalNo ratings yet
- Case Summaries For The MBBS StudentsDocument45 pagesCase Summaries For The MBBS StudentsAnmol KudalNo ratings yet
- Chronic Cough: IAP UG Teaching Slides 2015-16Document33 pagesChronic Cough: IAP UG Teaching Slides 2015-16Anmol KudalNo ratings yet
- Plaquenil Hydroxychloroquine Sulfate Tablets, UspDocument11 pagesPlaquenil Hydroxychloroquine Sulfate Tablets, UspAnmol KudalNo ratings yet
- Bidirectional COVID TBDocument2 pagesBidirectional COVID TBAnmol KudalNo ratings yet
- NEET PG 2020 Questions: (Memory Based)Document25 pagesNEET PG 2020 Questions: (Memory Based)Anmol KudalNo ratings yet
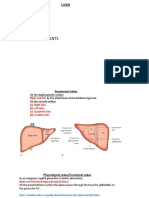
- 2 Surgical Lobes - 3 Minor Fissures - 3 Major Fissures - 4 Portal Sectors - 8 Functional SegmentsDocument9 pages2 Surgical Lobes - 3 Minor Fissures - 3 Major Fissures - 4 Portal Sectors - 8 Functional SegmentsAnmol KudalNo ratings yet
- Examination Heart Sounds and MurmursDocument52 pagesExamination Heart Sounds and MurmursAnmol KudalNo ratings yet
- Removal of Difficulties in Internship For Med Graduates MBBS PDFDocument2 pagesRemoval of Difficulties in Internship For Med Graduates MBBS PDFAnmol KudalNo ratings yet
- Tips For Final Year Mbbs PDFDocument6 pagesTips For Final Year Mbbs PDFAnmol KudalNo ratings yet
- 4 5789805297295950451 PDFDocument356 pages4 5789805297295950451 PDFAnmol Kudal100% (1)
- 4 CovidDocument47 pages4 CovidAbhishek toppoNo ratings yet
- Home - Impanelled Hospital ListDocument20 pagesHome - Impanelled Hospital ListeffefefeNo ratings yet
- ResumeDocument2 pagesResumeapi-283876119No ratings yet
- Omnibus Health Guidelines For Adults 2022Document99 pagesOmnibus Health Guidelines For Adults 2022Raymunda Rauto-avilaNo ratings yet
- CMS Place of Service Codes 2009Document6 pagesCMS Place of Service Codes 2009Rakshith KambleNo ratings yet
- Course Content:: What Does Tender Mean?Document13 pagesCourse Content:: What Does Tender Mean?Wahib WaqasNo ratings yet
- Literature Review On Health and Safety in The WorkplaceDocument8 pagesLiterature Review On Health and Safety in The WorkplaceafmzrvaxhdzxjsNo ratings yet
- Project Proposal: Department of Labor and EmploymentDocument2 pagesProject Proposal: Department of Labor and EmploymentinvictuslorenzoNo ratings yet
- Summit TM-40 MSDSDocument5 pagesSummit TM-40 MSDSVfuentes14No ratings yet
- CHN Lec Finals UpdatedDocument69 pagesCHN Lec Finals UpdatedShainaChescaEvansNo ratings yet
- Name: May Lyka O. Galit Grade & Section: 12 GAS-VILLADocument7 pagesName: May Lyka O. Galit Grade & Section: 12 GAS-VILLAGALIT, MAY LYKA O.No ratings yet
- Richard Et Al., (2022) Revisión de EstudiosDocument13 pagesRichard Et Al., (2022) Revisión de EstudiosAlicia BANo ratings yet
- Neural Plasticity 2020Document11 pagesNeural Plasticity 2020ANo ratings yet
- Wetland RoofsDocument9 pagesWetland Roofskloe-tran-6552No ratings yet
- CA Channel BlockersDocument19 pagesCA Channel BlockersanojanNo ratings yet
- Oleh: Heru Nurcahyo Magister Pendidikan Biologi Pps Uny 2019Document110 pagesOleh: Heru Nurcahyo Magister Pendidikan Biologi Pps Uny 2019RheaNo ratings yet
- 2014-07-03Document77 pages2014-07-03emwongera50% (2)
- PTW Sample-Control Oil SystemDocument2 pagesPTW Sample-Control Oil SystemdikiNo ratings yet
- Suman Das-1Document21 pagesSuman Das-1Susmita DuttaNo ratings yet
- 8 The Affective Neuroscience Personality Scales: Normative Data and ImplicationsDocument14 pages8 The Affective Neuroscience Personality Scales: Normative Data and ImplicationsMaximiliano PortilloNo ratings yet
- NCP 2Document3 pagesNCP 2romelyn100% (1)
- Drug AbreviationDocument14 pagesDrug AbreviationGlenn Suerte100% (1)
- Etiology of Acute Fever in COVID-19 Era SUS PDFDocument26 pagesEtiology of Acute Fever in COVID-19 Era SUS PDFIda Bagus Aditya NugrahaNo ratings yet
- Case Sis MelenaDocument26 pagesCase Sis MelenaAnnisa JuwitaNo ratings yet
- Configuration of Circle of Willis in Bangladeshi Population An Observational StudyDocument3 pagesConfiguration of Circle of Willis in Bangladeshi Population An Observational StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- THE Foodservice IndustryDocument84 pagesTHE Foodservice IndustryMunch RoomNo ratings yet
- CRMTCS 6.docx LEGAL MEDDocument7 pagesCRMTCS 6.docx LEGAL MEDRendell EusebioNo ratings yet