You might also like
- Principles and Practice of Systematic Reviews and Meta-AnalysisFrom EverandPrinciples and Practice of Systematic Reviews and Meta-AnalysisNo ratings yet
- Instrument AssesmentDocument11 pagesInstrument Assesmentyunita arbaniNo ratings yet
- Reviewon QualityassessmentDocument13 pagesReviewon QualityassessmentnewsPewNo ratings yet
- Migliavaca - Et.al.2020. Quality Assessment of Cross Sectional (Prevalence) Studies A Systematic ReviewDocument10 pagesMigliavaca - Et.al.2020. Quality Assessment of Cross Sectional (Prevalence) Studies A Systematic ReviewmichaellouisgrecoNo ratings yet
- Reviewing The Literature, How Systematic Is SystematicDocument10 pagesReviewing The Literature, How Systematic Is SystematicEtna VeraguasNo ratings yet
- Development of A Quantitative Scoring Method For Strobe ChecklistDocument13 pagesDevelopment of A Quantitative Scoring Method For Strobe Checklistgopi mistryNo ratings yet
- Tools For Assessing Methodological Quality of Observational Studies Pre-PrintDocument55 pagesTools For Assessing Methodological Quality of Observational Studies Pre-PrintLisa PrihastariNo ratings yet
- AMSTAR ArticlesDocument9 pagesAMSTAR ArticlesNur Ainatul AtiqahNo ratings yet
- Pai NMJI 2004 Systematic Reviews Illustrated Guide3Document10 pagesPai NMJI 2004 Systematic Reviews Illustrated Guide3mphil.rameshNo ratings yet
- Article Critical AppraisalDocument8 pagesArticle Critical AppraisalagdroubiNo ratings yet
- Optimising The Value of The Critical Appraisal SkiDocument12 pagesOptimising The Value of The Critical Appraisal SkiFirmanNo ratings yet
- LI, Meixuan Et Al. (2019)Document6 pagesLI, Meixuan Et Al. (2019)Rafael ConcursoNo ratings yet
- AMSTAR 2 A Critical Appraisal Tool For Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or BothDocument9 pagesAMSTAR 2 A Critical Appraisal Tool For Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or BothPedro AfonsoNo ratings yet
- AMSTAR Analise Critica BMJ 2017Document9 pagesAMSTAR Analise Critica BMJ 2017Elizoneth SessaNo ratings yet
- JBI Critical Appraisal-Checklist For Analytical Cross Sectional StudiesDocument6 pagesJBI Critical Appraisal-Checklist For Analytical Cross Sectional StudieslinlinNo ratings yet
- Assessing The Quality of Reports of Randomized Clinical Trials Is Blinding NecessaryDocument12 pagesAssessing The Quality of Reports of Randomized Clinical Trials Is Blinding NecessaryOrveNo ratings yet
- NHMRC Evidence Hierarchy Designations of Levels of Evidence' According To Type of Research Question (Including Explanatory Notes)Document21 pagesNHMRC Evidence Hierarchy Designations of Levels of Evidence' According To Type of Research Question (Including Explanatory Notes)varahamihirNo ratings yet
- Data Collection Instrument and Procedure For Systematic Reviews in The Guide To Community Preventive ServicesDocument32 pagesData Collection Instrument and Procedure For Systematic Reviews in The Guide To Community Preventive ServicesAbdur RaziqNo ratings yet
- A Guide To Systematic Literature ReviewsDocument4 pagesA Guide To Systematic Literature ReviewsUSM GohNo ratings yet
- A Practical Approach To Evidence-Based Dentistry: VIDocument12 pagesA Practical Approach To Evidence-Based Dentistry: VIDiego Pinto PatroniNo ratings yet
- 6-Evidence Based For Hinari UsersDocument58 pages6-Evidence Based For Hinari UsersMohmmed Abu MahadyNo ratings yet
- Amstar 2 RevisionDocument9 pagesAmstar 2 RevisionIvan ToscaniNo ratings yet
- Critical AppraisalDocument5 pagesCritical AppraisalIntan Kartika NursyahbaniNo ratings yet
- Critical Appraisal of Healthcare Literature GuideDocument2 pagesCritical Appraisal of Healthcare Literature GuideGenevieve LawrenceNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptMarvin BundoNo ratings yet
- AMSTAR 2 A Critical Appraisal Tool For Systematic Reviews ThatDocument9 pagesAMSTAR 2 A Critical Appraisal Tool For Systematic Reviews ThatbcvgbNo ratings yet
- Using Quality Assessment Tools To CriticallyDocument7 pagesUsing Quality Assessment Tools To Criticallyanuraag lohmrorNo ratings yet
- Jadad Scale PDFDocument12 pagesJadad Scale PDFEnaik100% (1)
- Non-Randomize Araştırma Değerlendirme ChecklistiDocument12 pagesNon-Randomize Araştırma Değerlendirme ChecklistiGizem Beycan EkitliNo ratings yet
- Systematic Review 508Document2 pagesSystematic Review 508SaiKai54No ratings yet
- Criterios de Evaluacion para La Inv. Cualitativa en Cuidado de SaludDocument9 pagesCriterios de Evaluacion para La Inv. Cualitativa en Cuidado de SaludeacoboNo ratings yet
- Part 17 PDFDocument6 pagesPart 17 PDFKarolina PolskaNo ratings yet
- Diferentes Diseños en MADocument18 pagesDiferentes Diseños en MAdianacas07No ratings yet
- BMC Medical Research MethodologyDocument7 pagesBMC Medical Research MethodologyCarolina EspinozaNo ratings yet
- Downs and Black (1998)Document8 pagesDowns and Black (1998)ASHISH KUMARNo ratings yet
- IJHR - Volume 3 - Issue 4 - Pages 199-208Document10 pagesIJHR - Volume 3 - Issue 4 - Pages 199-208Nehal KhalafNo ratings yet
- Research Study DesignsDocument12 pagesResearch Study DesignsDr Deepthi GillaNo ratings yet
- NHMRC Levels and Grades (2009) PDFDocument24 pagesNHMRC Levels and Grades (2009) PDFAININo ratings yet
- Reporting guidelines for qualitative research interviews and focus groupsDocument9 pagesReporting guidelines for qualitative research interviews and focus groupsNurul QalbyNo ratings yet
- Critical AppraisalDocument132 pagesCritical AppraisalSanditia Gumilang100% (2)
- BMC Medical Research MethodologyDocument7 pagesBMC Medical Research Methodologylorena sotoNo ratings yet
- Systematic Reviews in HealthcareDocument149 pagesSystematic Reviews in HealthcareTati AnaNo ratings yet
- COREQ CheckList Untuk Penelitian KualitatifDocument9 pagesCOREQ CheckList Untuk Penelitian KualitatifRosnidar SumardiNo ratings yet
- Evidence Based PracticeDocument28 pagesEvidence Based Practiceraghad awwadNo ratings yet
- 1471 2288 3 25Document14 pages1471 2288 3 25mweNo ratings yet
- Methods A Systematic Review of Measurement Properties of Instruments Assessing PresenteeismDocument15 pagesMethods A Systematic Review of Measurement Properties of Instruments Assessing Presenteeismtriannisa agitiyaNo ratings yet
- 1-S2.0-S1471595323001944-MainDocument10 pages1-S2.0-S1471595323001944-MainAndrada Marko PoloNo ratings yet
- Applying Psychological Frameworks of Behaviour Change To Improve Healthcare Worker Hand Hygiene: A Systematic ReviewDocument9 pagesApplying Psychological Frameworks of Behaviour Change To Improve Healthcare Worker Hand Hygiene: A Systematic ReviewAnonymous b6xAErNo ratings yet
- Difference Between Literature Review and MethodologyDocument6 pagesDifference Between Literature Review and MethodologyhfuwwbvkgNo ratings yet
- The Value of A Second Reviewer For Study Selection in Systematic ReviewsDocument7 pagesThe Value of A Second Reviewer For Study Selection in Systematic ReviewsJosé Carlos Sánchez-RamirezNo ratings yet
- How To Critically Appraise An Article1Document10 pagesHow To Critically Appraise An Article1Arindam MukherjeeNo ratings yet
- Tailieuxanh cc3803 0597Document8 pagesTailieuxanh cc3803 0597Cu ChíNo ratings yet
- Literature Review CochraneDocument7 pagesLiterature Review Cochranenywxluvkg100% (1)
- Critical Appraisal of Clinical ResearchDocument8 pagesCritical Appraisal of Clinical ResearchUmm E KulsoomNo ratings yet
- What Is A Systematic Literature Review DefinitionDocument5 pagesWhat Is A Systematic Literature Review Definitionfvf69dxt100% (1)
- Concise Biostatistical Principles & Concepts: Guidelines for Clinical and Biomedical ResearchersFrom EverandConcise Biostatistical Principles & Concepts: Guidelines for Clinical and Biomedical ResearchersNo ratings yet
- Development of Questionnaires for Quantitative Medical ResearchFrom EverandDevelopment of Questionnaires for Quantitative Medical ResearchNo ratings yet
- The Sourcebook for Clinical Research: A Practical Guide for Study ConductFrom EverandThe Sourcebook for Clinical Research: A Practical Guide for Study ConductRating: 5 out of 5 stars5/5 (1)
- Caffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index Among Medical Students in Chongqing, China: A Multiple Mediation ModelDocument12 pagesCaffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index Among Medical Students in Chongqing, China: A Multiple Mediation ModelRhael LopesNo ratings yet
- JBI Critical Appraisal-Checklist For Prevalence StudiesDocument8 pagesJBI Critical Appraisal-Checklist For Prevalence StudiesWahyu DnanikNo ratings yet
- Renderer InfoDocument1 pageRenderer Infoメアリー アナNo ratings yet
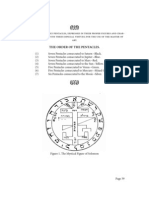
- Pentacles of SolomonDocument21 pagesPentacles of SolomonJoseph Burns100% (4)
- Read MeDocument1 pageRead MeRhael LopesNo ratings yet
- Strategic Marketing Plan for British American TobaccoDocument31 pagesStrategic Marketing Plan for British American TobaccoAli Abbas50% (2)
- CSS History of Indo Pak NotesDocument23 pagesCSS History of Indo Pak NotesASAD ULLAH100% (2)
- Scotts S2048 S2554 Operators ManualDocument99 pagesScotts S2048 S2554 Operators ManualobixmtNo ratings yet
- Guidelines SLCM BWDocument60 pagesGuidelines SLCM BWpnaarayanNo ratings yet
- Haloalkanes and Haloarenes Notes GoodDocument21 pagesHaloalkanes and Haloarenes Notes GoodAnitesh DharamNo ratings yet
- Using Previous Years AlmanacDocument1 pageUsing Previous Years AlmanacbhabhasunilNo ratings yet
- BCG ReportDocument9 pagesBCG Reportjlgjlj ljglkhNo ratings yet
- Sony STR Da80esDocument66 pagesSony STR Da80estelstarservicesNo ratings yet
- Project management software enables collaborationDocument4 pagesProject management software enables collaborationNoman AliNo ratings yet
- Summary G.E 9 Rizal Works (Chapter 1-13)Document23 pagesSummary G.E 9 Rizal Works (Chapter 1-13)Erwin Jay CabantacNo ratings yet
- CNC Instructables PDFDocument13 pagesCNC Instructables PDFNadim AhmedNo ratings yet
- Omega: Mahdi Alinaghian, Nadia ShokouhiDocument15 pagesOmega: Mahdi Alinaghian, Nadia ShokouhiMohcine ES-SADQINo ratings yet
- 5.test Report - RFU-C-7Ghz IP10 Extract VersionDocument42 pages5.test Report - RFU-C-7Ghz IP10 Extract Versionminhdung.pham4713No ratings yet
- Automation of Banking Service - EBL & EXIM BankDocument32 pagesAutomation of Banking Service - EBL & EXIM BankShaffyNo ratings yet
- "A Study Consumer Satisfaction Towards Royal Enfield BikesDocument72 pages"A Study Consumer Satisfaction Towards Royal Enfield BikesKotresh Kp100% (1)
- Bee WareDocument49 pagesBee WareJayNo ratings yet
- MMC Fiori Cheat Sheet PDFDocument2 pagesMMC Fiori Cheat Sheet PDFAleksandar KNo ratings yet
- Goethe Zertifikat b1 HorenDocument2 pagesGoethe Zertifikat b1 HorenLevent75% (4)
- Nord Stage Factory Patches v3 v4 v5Document18 pagesNord Stage Factory Patches v3 v4 v5Danilo Giuliani DobermannNo ratings yet
- LogDocument15 pagesLogandrew_hm925635No ratings yet
- Results and DiscussionsDocument13 pagesResults and DiscussionsEdpher Leo SindolNo ratings yet
- Building Lean Supply ChainsDocument33 pagesBuilding Lean Supply ChainsJefri MustaphaNo ratings yet
- Anxiety, Depression and Self-Esteem in Children With Well-Controlled AsthmaDocument6 pagesAnxiety, Depression and Self-Esteem in Children With Well-Controlled AsthmaAbdallah H. KamelNo ratings yet
- Mazda 6 2014 - Automatic Transaxle Workshop Manual FW6A-EL PDFDocument405 pagesMazda 6 2014 - Automatic Transaxle Workshop Manual FW6A-EL PDFFelipe CalleNo ratings yet
- (Culture and History of The Ancient Near East 65) Leslie Anne Warden - Pottery and Economy in Old Kingdom Egypt-Brill Academic Publishers (2014)Document343 pages(Culture and History of The Ancient Near East 65) Leslie Anne Warden - Pottery and Economy in Old Kingdom Egypt-Brill Academic Publishers (2014)HugoBotello100% (1)
- RRT LH: Gt'R:Ut (TLDocument75 pagesRRT LH: Gt'R:Ut (TLkl equipmentNo ratings yet
- Assessment Cover Sheet: BSB52415 Diploma of Marketing and Communication Student NameDocument11 pagesAssessment Cover Sheet: BSB52415 Diploma of Marketing and Communication Student NameChun Jiang0% (1)
- RLT-Guideline Certification: Herstellerverband Raumlufttechnische Geräte E. V. AHU Manufacturer AssociationDocument22 pagesRLT-Guideline Certification: Herstellerverband Raumlufttechnische Geräte E. V. AHU Manufacturer AssociationJorge RoblesNo ratings yet
- B.O Blog 6 (Benefits and Hacks of Using Turmeric)Document6 pagesB.O Blog 6 (Benefits and Hacks of Using Turmeric)sanaNo ratings yet
- Agile Spotify - Team - HomeworkDocument8 pagesAgile Spotify - Team - Homeworksp76rjm7dhNo ratings yet