You might also like
- Hospital and Critical CareDocument16 pagesHospital and Critical CareMarivy GalonNo ratings yet
- ACLS Practice Exam 1Document10 pagesACLS Practice Exam 1Ken Evans88% (16)
- Hospital and Critical CareDocument16 pagesHospital and Critical CareMarivy GalonNo ratings yet
- 200 Pages of MCQs LJDocument96 pages200 Pages of MCQs LJijojo elizabethNo ratings yet
- Pediatric Advanced Life Support (PALS) - UpToDateDocument51 pagesPediatric Advanced Life Support (PALS) - UpToDatenana100% (1)
- Surgery Absite CompilationDocument7 pagesSurgery Absite Compilationyayayaniza100% (1)
- 2) ERC Pre Course MCQDocument5 pages2) ERC Pre Course MCQS Vaibhav100% (2)
- 10-Platelet Structure and Function PDFDocument21 pages10-Platelet Structure and Function PDFAnil SharmaNo ratings yet
- ALS CPR and Defibrillation Assessment Sheet APR 20211 V1Document1 pageALS CPR and Defibrillation Assessment Sheet APR 20211 V1M Ismail100% (1)
- Essentials of Biostatistics - Second EdiDocument13 pagesEssentials of Biostatistics - Second EdiAnil Sharma0% (1)
- Defibrillation TypedDocument8 pagesDefibrillation TypedValarmathiNo ratings yet
- Bls - Fbao - First AidDocument172 pagesBls - Fbao - First AidMaria Regina Castro Gabriel100% (1)
- Final FrcaMCQ Mock Questions Feb2017Document15 pagesFinal FrcaMCQ Mock Questions Feb2017bobbykrishNo ratings yet
- Wrong Treatment During Resuscitation?Document13 pagesWrong Treatment During Resuscitation?adnan shw75% (4)
- 200 Pages of McqsDocument112 pages200 Pages of McqsSelim TarekNo ratings yet
- MCQ Int - MedDocument166 pagesMCQ Int - MedOmar Ahmed100% (1)
- MCQ Anaesthesia QuestionsDocument4 pagesMCQ Anaesthesia Questionsapi-2629165181% (32)
- Basic EcgDocument17 pagesBasic EcgJohn Vincent DerlaNo ratings yet
- Edan SE-3 User Manual V1-7Document75 pagesEdan SE-3 User Manual V1-7Fredi PanciNo ratings yet
- Medical Surgical Nursing Practice Test Part 1Document15 pagesMedical Surgical Nursing Practice Test Part 1cleznielNo ratings yet
- How To Pass Each ExaminationDocument50 pagesHow To Pass Each ExaminationBem PladeroNo ratings yet
- ACLS Pre Test AnswersDocument10 pagesACLS Pre Test AnswersAirene SibleNo ratings yet
- Midyear Exam 2011Document24 pagesMidyear Exam 2011Ghassan M ObaidNo ratings yet
- 278234155-Atls-Questions-and-Answers HHHHDocument14 pages278234155-Atls-Questions-and-Answers HHHHDyah Putri100% (1)
- Ekg QuestionsDocument18 pagesEkg QuestionsEvidence Chaibva100% (1)
- GP MCQ 3Document4 pagesGP MCQ 3Marta MoreiraNo ratings yet
- Implantable PacemakerDocument33 pagesImplantable PacemakerShifa Fauzia AfrianneNo ratings yet
- Storz Millenium Microsurgical System User ManualDocument188 pagesStorz Millenium Microsurgical System User ManualKaakaKhanNo ratings yet
- Nurse Exam QuestionsDocument3 pagesNurse Exam QuestionsrenjiniNo ratings yet
- Bexen Reanibex 700 Defibrillator - Technical Manual PDFDocument169 pagesBexen Reanibex 700 Defibrillator - Technical Manual PDFFábio Vitor Martins100% (1)
- Atls Questions and AnswersDocument14 pagesAtls Questions and Answersahmad7mahmoud-1No ratings yet
- ECG2350 EnglishSM 08SK2.006.00045BDocument102 pagesECG2350 EnglishSM 08SK2.006.00045BЮрій КобцевNo ratings yet
- Plab Emergency Medicine CompleteDocument141 pagesPlab Emergency Medicine CompleteSyedKashifAli100% (1)
- ACLS QuizletDocument7 pagesACLS Quizletek.9006001No ratings yet
- Multiple Choice Questions: DOI 10.1093/bjacepd/mkg125Document2 pagesMultiple Choice Questions: DOI 10.1093/bjacepd/mkg125Florence BamigbolaNo ratings yet
- Multiple Choice QuestionsDocument2 pagesMultiple Choice QuestionsChudaman Mahajan100% (1)
- Pi Is 1743181617300586Document4 pagesPi Is 1743181617300586Yasmin ElsisiNo ratings yet
- PIIS1743181617306170Document2 pagesPIIS1743181617306170Vikash KushwahaNo ratings yet
- 6 ShockDocument2 pages6 Shockعلاء محمدNo ratings yet
- Multiple Choice Questions: Anaesthesia For Major Spinal Surgery Paracetamol - Mechanisms and UpdatesDocument5 pagesMultiple Choice Questions: Anaesthesia For Major Spinal Surgery Paracetamol - Mechanisms and UpdatesFarhana RashenaNo ratings yet
- Ca 2 Cardiovascular-Oxygenation Assignment Part 1Document8 pagesCa 2 Cardiovascular-Oxygenation Assignment Part 1Joseph AbangNo ratings yet
- Staff Nurse Recruitment 2019 2020Document4 pagesStaff Nurse Recruitment 2019 2020renjiniNo ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsAppu JhaNo ratings yet
- Neurological (Reviewer)Document13 pagesNeurological (Reviewer)cataleya mesaNo ratings yet
- Multiple Choice Questions: Diagnosis of DeathDocument3 pagesMultiple Choice Questions: Diagnosis of DeathFaheem AfridiNo ratings yet
- Multiple Choice Questions: Chronic Obstructive Pulmonary Disease and Anaesthesia Anaesthesia For Awake CraniotomyDocument4 pagesMultiple Choice Questions: Chronic Obstructive Pulmonary Disease and Anaesthesia Anaesthesia For Awake CraniotomyEliza AmandoNo ratings yet
- GP MCQ 5Document4 pagesGP MCQ 5Marta MoreiraNo ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsNoor AhmedNo ratings yet
- Umum 2Document22 pagesUmum 2farid akbarNo ratings yet
- Multiple Choice Questions: Parenteral Nutrition in Critical CareDocument3 pagesMultiple Choice Questions: Parenteral Nutrition in Critical Careabhisheknrs78No ratings yet
- Multiple Choice Questions: Never Events: An Anaesthetic PerspectiveDocument4 pagesMultiple Choice Questions: Never Events: An Anaesthetic Perspectiveامین ثانیNo ratings yet
- Piis1743181617301890 PDFDocument4 pagesPiis1743181617301890 PDFZiaur RehmanNo ratings yet
- College Final Paper 1-3Document6 pagesCollege Final Paper 1-3Rita MoraaNo ratings yet
- Multiple Choice Questions: Preoperative Cardiopulmonary Exercise TestingDocument2 pagesMultiple Choice Questions: Preoperative Cardiopulmonary Exercise TestingdeadbysunriseeNo ratings yet
- GP MCQ 1Document4 pagesGP MCQ 1Marta MoreiraNo ratings yet
- GP MCQ 4Document4 pagesGP MCQ 4Marta MoreiraNo ratings yet
- GP MCQ 7Document4 pagesGP MCQ 7Marta MoreiraNo ratings yet
- Multiple Choice QuestionsDocument2 pagesMultiple Choice QuestionsAhmad FarhanNo ratings yet
- Mcqs 3Document12 pagesMcqs 3Noha AhmedNo ratings yet
- GP MCQ 9Document4 pagesGP MCQ 9Marta MoreiraNo ratings yet
- Practice QuestionDocument3 pagesPractice QuestionrenjiniNo ratings yet
- Coronary Artery Disease and Hypertension PDFDocument2 pagesCoronary Artery Disease and Hypertension PDFpaulzkieyyNo ratings yet
- Multiple Choice Questions: Preventing Postoperative Infection: The Anaesthetist's RoleDocument4 pagesMultiple Choice Questions: Preventing Postoperative Infection: The Anaesthetist's Roleiqra uroojNo ratings yet
- FPSC No: 55 Mcqs On Submission Deadline: 19 November 2013 12 NoonDocument4 pagesFPSC No: 55 Mcqs On Submission Deadline: 19 November 2013 12 Noonhassanmurtazashah33No ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsBiph BiphNo ratings yet
- Pharma Cardio Respi and Repro NclexdocxDocument8 pagesPharma Cardio Respi and Repro NclexdocxJhayneNo ratings yet
- Multiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006Document3 pagesMultiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006AatekaNo ratings yet
- Multiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006Document3 pagesMultiple Choice Questions: Continuing Education in Anaesthesia, Critical Care & Pain - Volume 6 Number 3 2006Maheen XhykhNo ratings yet
- Understanding The Essentials of Critical Care Nursing 3rd Edition Perrin Test BankDocument9 pagesUnderstanding The Essentials of Critical Care Nursing 3rd Edition Perrin Test Bankleonardedanah7lkhe100% (24)
- Multiple Choice Questions: Traumatic Brain Injury: An Evidence-Based Review of ManagementDocument5 pagesMultiple Choice Questions: Traumatic Brain Injury: An Evidence-Based Review of Managementaftab alamNo ratings yet
- Multiple Choice QuestionsDocument3 pagesMultiple Choice QuestionsRavi PulaNo ratings yet
- PTC MCQDocument7 pagesPTC MCQYevan HarryBrata0% (1)
- MedSurg A1Document16 pagesMedSurg A1ELAINE ESTRERANo ratings yet
- Transport System in India PDF For SSC RRB All Competitive ExamsDocument18 pagesTransport System in India PDF For SSC RRB All Competitive ExamsAnil SharmaNo ratings yet
- Vital StaticsDocument33 pagesVital StaticsAnil SharmaNo ratings yet
- Assistant Commissioner (Direct)Document120 pagesAssistant Commissioner (Direct)Anil SharmaNo ratings yet
- Page 8Document1 pagePage 8Anil SharmaNo ratings yet
- General Science: Career Point ShimlaDocument48 pagesGeneral Science: Career Point ShimlaAnil SharmaNo ratings yet
- Junior Assistant Syllabus PDFDocument29 pagesJunior Assistant Syllabus PDFAnil SharmaNo ratings yet
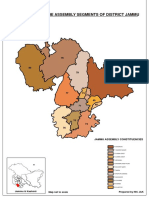
- Map Showing The Assembly Segments of District JammuDocument1 pageMap Showing The Assembly Segments of District JammuAnil SharmaNo ratings yet
- New Doc 2018 06 24 PDFDocument20 pagesNew Doc 2018 06 24 PDFAnil SharmaNo ratings yet
- Paediatics MCQDocument33 pagesPaediatics MCQAnil SharmaNo ratings yet
- PALS Guidelines For HypotensionDocument19 pagesPALS Guidelines For HypotensionAnil SharmaNo ratings yet
- Syllabus of Post Graduate Courses MD-MS-MCHDocument365 pagesSyllabus of Post Graduate Courses MD-MS-MCHAnil SharmaNo ratings yet
- Dokumen - Pub - Target Jipmer Dec 2018 9811156083 9788184452662 PDFDocument216 pagesDokumen - Pub - Target Jipmer Dec 2018 9811156083 9788184452662 PDFAnil SharmaNo ratings yet
- Data Communication and TerminologiesDocument8 pagesData Communication and TerminologiesAnil SharmaNo ratings yet
- DM Cardiology (Medicine) June 2018 PDFDocument17 pagesDM Cardiology (Medicine) June 2018 PDFAnil SharmaNo ratings yet
- C Pointers: Systems ProgrammingDocument20 pagesC Pointers: Systems ProgrammingAnil SharmaNo ratings yet
- CCC CPR AED Community Training GenericDocument18 pagesCCC CPR AED Community Training GenericDev Dutt Dey100% (1)
- PLUS Defibrillator CatalogueDocument2 pagesPLUS Defibrillator CataloguebogdasusNo ratings yet
- Trends in Medical Device Design and ManufacturingDocument6 pagesTrends in Medical Device Design and ManufacturingKatlheen Krautz تNo ratings yet
- Post Resuscitation CareDocument3 pagesPost Resuscitation CareprashsubbuNo ratings yet
- Pro Biphasic Defibrillator CatalogueDocument2 pagesPro Biphasic Defibrillator CatalogueMark D.No ratings yet
- Respiration AssessmentDocument7 pagesRespiration AssessmentWen RodsaNo ratings yet
- Erc - Sva 2021Document37 pagesErc - Sva 2021Vinícius MenegatNo ratings yet
- ACLSDocument275 pagesACLSShajahan SideequeNo ratings yet
- Comen Patient-Cardiac MonitorDocument2 pagesComen Patient-Cardiac Monitorjef1234321No ratings yet
- CPRDocument41 pagesCPRPreethi BNo ratings yet
- Dre Vidastat DM DefibrillatorDocument3 pagesDre Vidastat DM DefibrillatorWarut SeansukNo ratings yet
- Pediatric Cardiopulmonary ResuscitationDocument15 pagesPediatric Cardiopulmonary ResuscitationGhiza Ainurrahmah BawafieNo ratings yet
- P.E 1 Basic Life Support (BLS) 1: Check For ResponsivenessDocument5 pagesP.E 1 Basic Life Support (BLS) 1: Check For ResponsivenessThea GailNo ratings yet
- JSS JSS-2150/2150N 2150/2150N - 2250/2250N - 2250/2250N - 2500/2500N - 2500/2500NDocument248 pagesJSS JSS-2150/2150N 2150/2150N - 2250/2250N - 2250/2250N - 2500/2500N - 2500/2500NTuấn Pham MinhNo ratings yet
- Schiller At-3 ECG - User ManualDocument92 pagesSchiller At-3 ECG - User ManualStewO101 worcNo ratings yet
- 2.500428 0611 en Defigard 5000 LQDocument4 pages2.500428 0611 en Defigard 5000 LQGuillermo PortugalNo ratings yet
- M4137-A 02-11 - Effecta Technical ManualDocument128 pagesM4137-A 02-11 - Effecta Technical Manualzava2007No ratings yet
- Marquette Solar9500 - Service ManualDocument208 pagesMarquette Solar9500 - Service ManualElectromedicina CatanNo ratings yet