You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- The Definition of Death - S. Younger, Et Al (Johns Hopkins Univ) WW PDFDocument369 pagesThe Definition of Death - S. Younger, Et Al (Johns Hopkins Univ) WW PDFMunteanu AlexandruNo ratings yet
- Assimil - German Without Toil (1965)Document208 pagesAssimil - German Without Toil (1965)Zsa ZsuzsaNo ratings yet
- Review Article Ocular Myasthenia Gravis: A Review: Epidemiology and DemographicsDocument7 pagesReview Article Ocular Myasthenia Gravis: A Review: Epidemiology and DemographicsMaxend Arselino SilooyNo ratings yet
- Myasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaDocument9 pagesMyasthenia Gravis in Clinical Practice: Miastenia Gravis Na Prática ClínicaMasDhedotNo ratings yet
- 2 Myasthenia Gravis and MS 2Document50 pages2 Myasthenia Gravis and MS 2Rawbeena RamtelNo ratings yet
- PharmaDocument9 pagesPharmaمحسن حدوان عليخانNo ratings yet
- Acquired Demyelinating SyndromesDocument13 pagesAcquired Demyelinating SyndromesfbonillaNo ratings yet
- Diagnosis and Management of Myasthenia Gravis: ReviewDocument9 pagesDiagnosis and Management of Myasthenia Gravis: ReviewnetifarhatiiNo ratings yet
- Ni 09039Document8 pagesNi 09039Tomi NugrahaNo ratings yet
- 35 - Neuromuscular Junction Disorders LectureDocument45 pages35 - Neuromuscular Junction Disorders LectureRanjit SharmaNo ratings yet
- Smith2017 Ocular MGDocument9 pagesSmith2017 Ocular MGMunteanu AlexandruNo ratings yet
- Tjo 8 67Document7 pagesTjo 8 67Lissaberti AmaliahNo ratings yet
- E RefdDocument13 pagesE RefdGabriella TjondroNo ratings yet
- A Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosisDocument7 pagesA Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosistiaraleshaNo ratings yet
- 51.differential Diagnosis of Myasthenia Gravis - A ReviewDocument11 pages51.differential Diagnosis of Myasthenia Gravis - A ReviewSeptime TyasNo ratings yet
- Neuromyelitis Optica Spectrum Disorders.15Document33 pagesNeuromyelitis Optica Spectrum Disorders.15Marco Macavilca CruzNo ratings yet
- Neuromyelitis Optica (Devic's Syndrome) : An Appraisal: Vasculitis (LR Espinoza, Section Editor)Document9 pagesNeuromyelitis Optica (Devic's Syndrome) : An Appraisal: Vasculitis (LR Espinoza, Section Editor)ezradamanikNo ratings yet
- Journal Reading 3 - NODocument6 pagesJournal Reading 3 - NOezradamanikNo ratings yet
- Multifocal Motor Neuropathy - StatPearls - NCBI BookshelfDocument6 pagesMultifocal Motor Neuropathy - StatPearls - NCBI BookshelfAnakin SkywalkerNo ratings yet
- A Case of Neuromyelitis Optica (Devic's Disease)Document3 pagesA Case of Neuromyelitis Optica (Devic's Disease)Keisha QuinnNo ratings yet
- Neuromyelitisoptica: Sarah L. Patterson,, Sarah E. GoglinDocument13 pagesNeuromyelitisoptica: Sarah L. Patterson,, Sarah E. GoglinErji K.No ratings yet
- Pediatric Myasthenia Gravis: PathophysiologyDocument6 pagesPediatric Myasthenia Gravis: PathophysiologyLissaberti AmaliahNo ratings yet
- Pathogenesis of Opsoclonus MyoclonusDocument2 pagesPathogenesis of Opsoclonus MyoclonusIRENA GENINo ratings yet
- Update On Ocular Myasthenia GravisDocument12 pagesUpdate On Ocular Myasthenia GravisAnonymous QLadTClydkNo ratings yet
- Spinal Muscular Atrophy 2023Document21 pagesSpinal Muscular Atrophy 2023Arbey Aponte PuertoNo ratings yet
- Neuromyelitis Optica: Mark J. Morrow, MD, Dean Wingerchuk, MD, MSC, FRCP (C)Document13 pagesNeuromyelitis Optica: Mark J. Morrow, MD, Dean Wingerchuk, MD, MSC, FRCP (C)sidogra100% (1)
- Ratchford 2009Document8 pagesRatchford 2009Alfredo Enrique Marin AliagaNo ratings yet
- Per A Gallo 2017Document6 pagesPer A Gallo 2017Lissaberti AmaliahNo ratings yet
- Autoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityDocument16 pagesAutoimmune Myasthenia Gravis: Emerging Clinical and Biological HeterogeneityGiuseppeNo ratings yet
- MG 2Document5 pagesMG 2vaishnaviNo ratings yet
- Myasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaDocument31 pagesMyasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaIstván MáthéNo ratings yet
- MG Desya BismillahDocument20 pagesMG Desya BismillahDesya BillaNo ratings yet
- Esclerosis Multiple Presentación Clínica 2014Document22 pagesEsclerosis Multiple Presentación Clínica 2014Miguel HernandezNo ratings yet
- Corneal Sensitivity Myasthenia GravisDocument3 pagesCorneal Sensitivity Myasthenia GravisGemilang KhusnurrokhmanNo ratings yet
- Step 7 1. Mengapa Pada Skenario Pasien Merasakan Lemah Pada Kelopak Mata Dan Mengapa Paling Berat Dirasakan?Document11 pagesStep 7 1. Mengapa Pada Skenario Pasien Merasakan Lemah Pada Kelopak Mata Dan Mengapa Paling Berat Dirasakan?novkar9No ratings yet
- Autoimmune and Paraneoplastic MyeloDocument12 pagesAutoimmune and Paraneoplastic MyeloSimply SamNo ratings yet
- Myasthenia ParkinsonDocument44 pagesMyasthenia ParkinsonElena moralesNo ratings yet
- Referat MG Desya BismillahDocument20 pagesReferat MG Desya BismillahDesya BillaNo ratings yet
- Optic Neuritis in Leprosy - 231215 - 030338Document2 pagesOptic Neuritis in Leprosy - 231215 - 030338dr samyNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Nejmra 1904655Document9 pagesNejmra 1904655silviaNo ratings yet
- Journal of Autoimmunity: Sonia Berrih-Aknin, Rozen Le PanseDocument11 pagesJournal of Autoimmunity: Sonia Berrih-Aknin, Rozen Le PanseHelen SobczykNo ratings yet
- Jurnal GBSDocument15 pagesJurnal GBSfajar sugandaNo ratings yet
- Toosy Lancet Neurology 2014Document17 pagesToosy Lancet Neurology 2014Dirga Rasyidin LNo ratings yet
- A Review On Spinal Muscular Atrophy Clinical Classification, Etiology, Diagnosis and TreatmentDocument4 pagesA Review On Spinal Muscular Atrophy Clinical Classification, Etiology, Diagnosis and TreatmentEditor IJTSRDNo ratings yet
- Multiple SclerosisDocument4 pagesMultiple SclerosisMarwan M.No ratings yet
- Pérdida Aguda VisualDocument7 pagesPérdida Aguda VisualYanina Pérez de VillarrealNo ratings yet
- Acute Transverse Myelitis: Is The "Idiopathic" Form Vanishing?Document3 pagesAcute Transverse Myelitis: Is The "Idiopathic" Form Vanishing?anak99No ratings yet
- Myasthenia Gravis Etiology, Pathophysiology, Symptoms, Management and ComplicationsDocument15 pagesMyasthenia Gravis Etiology, Pathophysiology, Symptoms, Management and ComplicationsHidenNo ratings yet
- Motor Endplate Disorders Myasthenia Gravis Overview and DefinitionDocument4 pagesMotor Endplate Disorders Myasthenia Gravis Overview and DefinitionPJHGNo ratings yet
- Myathenis Gravis - 1St Draft: 3. Diagnosis and Symptomatology 3.1. SymptomatologyDocument4 pagesMyathenis Gravis - 1St Draft: 3. Diagnosis and Symptomatology 3.1. SymptomatologyAxl0No ratings yet
- GBS A ReviewDocument6 pagesGBS A ReviewNurul Kartika SariNo ratings yet
- Myasthenia GravisDocument11 pagesMyasthenia GravisSandeepSethiNo ratings yet
- Symposium Management of Optic Neuritis: Vimla Menon, Rohit Saxena, Ruby Misra, Swati PhuljheleDocument7 pagesSymposium Management of Optic Neuritis: Vimla Menon, Rohit Saxena, Ruby Misra, Swati PhuljheleHermawan LimNo ratings yet
- Treatment Guidelines of Chronic Inflammatory Demyelinating Polyneuropathy in ChinaDocument4 pagesTreatment Guidelines of Chronic Inflammatory Demyelinating Polyneuropathy in Chinajacinto isaac galvez cortezNo ratings yet
- Current Concept of Neuromyelitis Optica (NMO) and NMO Spectrum DisordersDocument10 pagesCurrent Concept of Neuromyelitis Optica (NMO) and NMO Spectrum DisordersGabriella TjondroNo ratings yet
- Profound Olfactory Dysfunction in Myasthenia GravisDocument5 pagesProfound Olfactory Dysfunction in Myasthenia GravisAngie Sidney Naranjo GarciaNo ratings yet
- JCM 13 01971Document11 pagesJCM 13 01971kkeryanNo ratings yet
- Oct 3Document15 pagesOct 3Star LadyNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Pathophysiology and Immunological Profile of Myasthenia Gravis and Its SubgroupsDocument5 pagesPathophysiology and Immunological Profile of Myasthenia Gravis and Its SubgroupsMunteanu AlexandruNo ratings yet
- Smith2017 Ocular MGDocument9 pagesSmith2017 Ocular MGMunteanu AlexandruNo ratings yet
- Neuromuscular Junction DisordersDocument20 pagesNeuromuscular Junction DisordersMunteanu AlexandruNo ratings yet
- Tong2018 Durere Si SimturiDocument8 pagesTong2018 Durere Si SimturiMunteanu AlexandruNo ratings yet
- Research 2 UtzDocument22 pagesResearch 2 UtzNER CARLO SANTOSNo ratings yet
- Examination of Eye PT IIDocument77 pagesExamination of Eye PT IIMihaela TomaNo ratings yet
- INI-CET 2020 ALL Solutions FULL-MergedDocument119 pagesINI-CET 2020 ALL Solutions FULL-MergedDr ajay purushottamNo ratings yet
- Orthopedic Physical Examination (DR - Bayu)Document45 pagesOrthopedic Physical Examination (DR - Bayu)Ghisca Chairiyah AmiNo ratings yet
- Pregnancy PlannerDocument75 pagesPregnancy PlannerDaniza LanyonNo ratings yet
- Bibliografie Cazuri DificileDocument2 pagesBibliografie Cazuri DificileParvan EugenNo ratings yet
- Drug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility BetahistineDocument16 pagesDrug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility Betahistineclydell joyce masiarNo ratings yet
- Whistleblower (20.05.2023)Document743 pagesWhistleblower (20.05.2023)piotrszewczyklondon100% (1)
- Discharge PlanDocument3 pagesDischarge PlanpsychyzeNo ratings yet
- Albumin Solution - Drug Information - UpToDateDocument15 pagesAlbumin Solution - Drug Information - UpToDateSuci WijayaNo ratings yet
- Diabetes ElektifDocument7 pagesDiabetes ElektifSiti SofiaNo ratings yet
- Dialysis BasicsDocument23 pagesDialysis Basicsdidik_sugiarto_2100% (1)
- Department of Education Grade 8 Euclid: JULY 8, 2022Document9 pagesDepartment of Education Grade 8 Euclid: JULY 8, 2022SHAIRUZ DUGAYNo ratings yet
- Ncbi - Nlm.nih - Gov-Pediatric PneumoniaDocument10 pagesNcbi - Nlm.nih - Gov-Pediatric Pneumoniako naythweNo ratings yet
- GRM International, Inc. Hiv/Aids Workplace Policy and ProgramDocument4 pagesGRM International, Inc. Hiv/Aids Workplace Policy and ProgramAlyssa Mae SulpicoNo ratings yet
- Pediatric MCQDocument17 pagesPediatric MCQAhmed Kassem100% (1)
- Phenol - Medical Management Guidelines - Toxic Substance Portal - ATSDR. (N.D.) - Agency ForDocument2 pagesPhenol - Medical Management Guidelines - Toxic Substance Portal - ATSDR. (N.D.) - Agency ForREBEKAH EQUIZNo ratings yet
- Oral Sensorimotor Therapy in Pediatric DysphagiaDocument1 pageOral Sensorimotor Therapy in Pediatric Dysphagiashaghala38No ratings yet
- MSE AssingmentDocument5 pagesMSE AssingmentTumaini LifaNo ratings yet
- Signs and Symptoms: Pathophysiology Concept MapDocument1 pageSigns and Symptoms: Pathophysiology Concept MapAngela Mae DiestroNo ratings yet
- Kanner AutismDocument5 pagesKanner AutismNinelys CodNo ratings yet
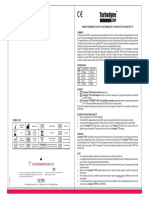
- Turbodyne: Tulip Diagnostics (P) LTDDocument2 pagesTurbodyne: Tulip Diagnostics (P) LTDMatibar RahmanNo ratings yet
- Gram Positive RodsDocument74 pagesGram Positive RodsSophia E. BucarileNo ratings yet
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- TeratomaDocument13 pagesTeratomaGoncang Setyo PambudiNo ratings yet
- AmenorrheaDocument51 pagesAmenorrheabisharatNo ratings yet
- Eating DisordersDocument63 pagesEating Disordersamir ARSHADNo ratings yet
- Supraventricular Tachycardia NotesDocument59 pagesSupraventricular Tachycardia NotesShadi TabbarahNo ratings yet
- Literature Review CD HLTH 634Document8 pagesLiterature Review CD HLTH 634api-518080609No ratings yet
- Harsh PatientReportDocument1 pageHarsh PatientReportHarsh GuptaNo ratings yet