You might also like
- Post-Viral Effects of COVID-19 in The Olfactory System and Their ImplicationsDocument9 pagesPost-Viral Effects of COVID-19 in The Olfactory System and Their ImplicationsJorge Augusto Israel 狼No ratings yet
- An Investigation Into The WIV Databases That Were Taken of IneDocument26 pagesAn Investigation Into The WIV Databases That Were Taken of InelaotanNo ratings yet
- English 9 Activity Sheet: Quarter 3 - MELC 3Document9 pagesEnglish 9 Activity Sheet: Quarter 3 - MELC 3rai genolos67% (9)
- Contingency Plan: Madapdap Resettlement High SchoolDocument12 pagesContingency Plan: Madapdap Resettlement High SchoolHacky Tot100% (2)
- Mckinsey Report - COVID-19-Facts-and-Insights-March-25 PDFDocument57 pagesMckinsey Report - COVID-19-Facts-and-Insights-March-25 PDFUmang K100% (2)
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- 1 s2.0 S2213260020302435 MainDocument6 pages1 s2.0 S2213260020302435 MainranauliafkNo ratings yet
- Journal Pre-Proof: JACC: Basic To Translational ScienceDocument6 pagesJournal Pre-Proof: JACC: Basic To Translational ScienceAjideniNo ratings yet
- Journal Pre-Proof: Best Practice & Research Clinical AnaesthesiologyDocument62 pagesJournal Pre-Proof: Best Practice & Research Clinical AnaesthesiologyMohammed Shuaib AhmedNo ratings yet
- Outcomes and Risk Factors For Cardiovascular Events in Hospitalized COVID-19 PatientsDocument13 pagesOutcomes and Risk Factors For Cardiovascular Events in Hospitalized COVID-19 Patientslaura_d_2No ratings yet
- PIIS0140673622003270Document7 pagesPIIS0140673622003270chaivat kNo ratings yet
- SARS-CoV-2 Viremia Is Associated With Distinct Proteomic Pathways and Predicts COVID-19 OutcomesDocument13 pagesSARS-CoV-2 Viremia Is Associated With Distinct Proteomic Pathways and Predicts COVID-19 OutcomesYoga Nugraha WNo ratings yet
- A Rampage Through: The BodyDocument5 pagesA Rampage Through: The BodyEdmundo CadilhaNo ratings yet
- 2021 - Ochoa Et Al - HCWDocument43 pages2021 - Ochoa Et Al - HCWMario Martínez TorijaNo ratings yet
- Covid-19 in Critically Ill Patients in The Seattle Region - Case SeriesDocument18 pagesCovid-19 in Critically Ill Patients in The Seattle Region - Case SeriesZelgi PutraNo ratings yet
- Journal of Critical CareDocument5 pagesJournal of Critical CareUnomoshNo ratings yet
- Jama Sanders 2020 RV 200005 PDFDocument13 pagesJama Sanders 2020 RV 200005 PDFPuty Annisa PrilinaNo ratings yet
- Jama Sanders 2020 RV 200005Document13 pagesJama Sanders 2020 RV 200005nanaNo ratings yet
- Sepsis and Septic Shock: June 2016Document22 pagesSepsis and Septic Shock: June 2016FriskaNo ratings yet
- Jurnal Covid 19Document46 pagesJurnal Covid 19Adeta Yuniza100% (1)
- Ni Hms 794087Document24 pagesNi Hms 794087Croitoru CosminNo ratings yet
- Critical Care For Multiple Organ Failure SecondaryDocument20 pagesCritical Care For Multiple Organ Failure SecondarysazaperdanaNo ratings yet
- COVID-19-Induced Neurovascular Injury: A Case Series With Emphasis On Pathophysiological MechanismsDocument17 pagesCOVID-19-Induced Neurovascular Injury: A Case Series With Emphasis On Pathophysiological MechanismsAji Prasetyo UtomoNo ratings yet
- Artigo Pra Ler 2Document27 pagesArtigo Pra Ler 2Luiz ClaudioNo ratings yet
- 2.prevalence and Impact of - Myocardial InjuryDocument14 pages2.prevalence and Impact of - Myocardial Injuryrest_a2003No ratings yet
- MainDocument9 pagesMainDeny NoviantoroNo ratings yet
- Price Et Al, Hospitalization and Mortality Among Black Patients and White Patients With Covid-19Document10 pagesPrice Et Al, Hospitalization and Mortality Among Black Patients and White Patients With Covid-19Constanzza Arellano LeivaNo ratings yet
- 20220623135722-Artigo - Covid 19 e OutrasoençasDocument43 pages20220623135722-Artigo - Covid 19 e Outrasoençasmarcos crescencioNo ratings yet
- Sphingomonas KoreensisDocument11 pagesSphingomonas KoreensisSMIBA MedicinaNo ratings yet
- Definition of SIRS, Sepsis, Severe SepsisDocument9 pagesDefinition of SIRS, Sepsis, Severe SepsisSara NicholsNo ratings yet
- New Insights of Emerging Sars-Cov-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and PreventionDocument22 pagesNew Insights of Emerging Sars-Cov-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and PreventionWendi IochNo ratings yet
- Predictors of COVID-19 Severity: A Literature ReviewDocument10 pagesPredictors of COVID-19 Severity: A Literature ReviewRafiqua Sifat JahanNo ratings yet
- Journal Pre-Proof: Diagnostic Microbiology & Infectious DiseaseDocument97 pagesJournal Pre-Proof: Diagnostic Microbiology & Infectious DiseaseLuis AlbertoNo ratings yet
- HHS Public Access: The Third International Consensus Definitions For Sepsis and Septic Shock (Sepsis-3)Document24 pagesHHS Public Access: The Third International Consensus Definitions For Sepsis and Septic Shock (Sepsis-3)graciasNo ratings yet
- Chronic Medical Conditions and Risk of SepsisDocument7 pagesChronic Medical Conditions and Risk of SepsisMargarita RamirezNo ratings yet
- KWF 113Document11 pagesKWF 113Residentes RadiologiaHCENo ratings yet
- Journal Pre-Proof: Journal of Cardiothoracic and Vascular AnesthesiaDocument36 pagesJournal Pre-Proof: Journal of Cardiothoracic and Vascular AnesthesiaBotez MartaNo ratings yet
- Molecular Dissection of Chagas Induced CardiomyopathyDocument31 pagesMolecular Dissection of Chagas Induced CardiomyopathyClaudia Calvet AlvarezNo ratings yet
- Tocilizumab en Covid 19Document12 pagesTocilizumab en Covid 19Frank Antony Arizabal GaldosNo ratings yet
- 10.5811@westjem.2020.6.47919 (2) 81105Document7 pages10.5811@westjem.2020.6.47919 (2) 81105Giovan GaulNo ratings yet
- Ruan2020 Article ClinicalPredictorsOfMortalityDDocument3 pagesRuan2020 Article ClinicalPredictorsOfMortalityDntnquynhproNo ratings yet
- The Natural History, Pathobiology, and Clinical Manifestations of Sars-Cov-2 InfectionsDocument28 pagesThe Natural History, Pathobiology, and Clinical Manifestations of Sars-Cov-2 InfectionsJosé Luis Alonso EscamillaNo ratings yet
- Hpaa 057Document2 pagesHpaa 057RISMA ARLYANINo ratings yet
- Emerging Infectious Disease Agents and Their Potential Threat To Transfusion Safety.Document29 pagesEmerging Infectious Disease Agents and Their Potential Threat To Transfusion Safety.Pritha BhuwapaksophonNo ratings yet
- Excellent Paper On Covid 19Document20 pagesExcellent Paper On Covid 19GalenNo ratings yet
- CrothersDocument8 pagesCrothersMETA INVESTIGACIÓN Y DESARROLLONo ratings yet
- NEJM. COVID CHINA. 10.1056@NEJMoa2002032Document13 pagesNEJM. COVID CHINA. 10.1056@NEJMoa2002032Boris CabreraNo ratings yet
- Jama Sanders 2020 RV 200005Document13 pagesJama Sanders 2020 RV 200005Benjamin Rodriguez CabreraNo ratings yet
- The Novel Coronavirus' Spike Protein Plays Additional Key Role in Illness - Salk Institute For Biological StudiesDocument4 pagesThe Novel Coronavirus' Spike Protein Plays Additional Key Role in Illness - Salk Institute For Biological StudieschingatchgookNo ratings yet
- Ali 01Document10 pagesAli 01Juan Fernando Garcia RobledoNo ratings yet
- COVID-19 and Multi-Organ ResponseDocument31 pagesCOVID-19 and Multi-Organ ResponseArbaz SultanNo ratings yet
- The Emergence and Persistence of C Auris in Western New YorkDocument4 pagesThe Emergence and Persistence of C Auris in Western New YorkLilia JouNo ratings yet
- BBA - Molecular Basis of Disease: ReviewDocument12 pagesBBA - Molecular Basis of Disease: ReviewautomationenggNo ratings yet
- Correspondence: Smell and Taste Dysfunction in Patients With COVID-19Document1 pageCorrespondence: Smell and Taste Dysfunction in Patients With COVID-19Dhyo Asy-shidiq HasNo ratings yet
- HHS Public Access: HypertensionDocument48 pagesHHS Public Access: HypertensionFarmasi RSUD Kramat JatiNo ratings yet
- A miRNA PEPTIDE FUSION AS A VACCINE CANDIDATE AGAINSTCOVID 19Document12 pagesA miRNA PEPTIDE FUSION AS A VACCINE CANDIDATE AGAINSTCOVID 19Pipirrin GonzalesNo ratings yet
- Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19Document15 pagesPrognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19Basilio BabarNo ratings yet
- Articulo Cientifico Derrame Pleural en Covid 19Document10 pagesArticulo Cientifico Derrame Pleural en Covid 19Leyla Barnard LagunaNo ratings yet
- Zhu2020 Article CardiovascularComplicationsInPDocument9 pagesZhu2020 Article CardiovascularComplicationsInPJRDEABREUNo ratings yet
- Jce 30035Document7 pagesJce 30035Sridevi DinakaranNo ratings yet
- Combing Through Traditional Texts To Prevent Covid-19 - A Scientific ApproachDocument14 pagesCombing Through Traditional Texts To Prevent Covid-19 - A Scientific ApproachVinayNo ratings yet
- DeSanto 3057Document8 pagesDeSanto 3057Maryka CociuNo ratings yet
- ABO Blood Type Association With SARS CoV 2 Infection Mortality 2021Document7 pagesABO Blood Type Association With SARS CoV 2 Infection Mortality 2021azizk83No ratings yet
- Raynaud’s Phenomenon: A Guide to Pathogenesis and TreatmentFrom EverandRaynaud’s Phenomenon: A Guide to Pathogenesis and TreatmentFredrick M. WigleyNo ratings yet
- Memo - COVID-19 Vaccine Distribution UpdateDocument7 pagesMemo - COVID-19 Vaccine Distribution UpdateCTV Ottawa100% (1)
- Office of The Punong Barangay Executive Order No. 03Document2 pagesOffice of The Punong Barangay Executive Order No. 03pablo gayodanNo ratings yet
- Dealing With Second Wave of Covid - 19Document11 pagesDealing With Second Wave of Covid - 19Sajith KumarNo ratings yet
- Activity Sheet Practical Research 1 Group 1Document28 pagesActivity Sheet Practical Research 1 Group 1SRHeart Nikcole Dela PazNo ratings yet
- Weekly CT-performance-monitoring-toolDocument1 pageWeekly CT-performance-monitoring-toolJurryNo ratings yet
- Waiver For Independent ContractorsDocument2 pagesWaiver For Independent ContractorsChristian Roque0% (1)
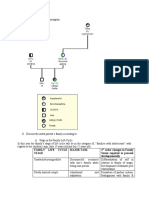
- Family Life Cycle Stage Major Task 2 Order Changes in Family Status Required To Proceed DevelopmentallyDocument6 pagesFamily Life Cycle Stage Major Task 2 Order Changes in Family Status Required To Proceed DevelopmentallyAris Jasper NacionNo ratings yet
- Renata 2019-2020Document194 pagesRenata 2019-2020Nayyab Alam TurjoNo ratings yet
- HOO - Coronavirus - Blanket - Isolation 7 1 20Document3 pagesHOO - Coronavirus - Blanket - Isolation 7 1 20mattbettNo ratings yet
- Acceptance and Attitude Toward Covid-19 Vaccination: A Cross-Sectional Study From Udaipur DistrictDocument8 pagesAcceptance and Attitude Toward Covid-19 Vaccination: A Cross-Sectional Study From Udaipur DistrictIJAR JOURNALNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- Acquired Immuno Deficiency Syndrome (Aids)Document9 pagesAcquired Immuno Deficiency Syndrome (Aids)alina20No ratings yet
- Effectiveness of Whatsapp For Blood Donor Mobilization Campaigns During Covid-19 PandemicDocument5 pagesEffectiveness of Whatsapp For Blood Donor Mobilization Campaigns During Covid-19 PandemicBala BhaskarNo ratings yet
- D Properties Covid 19 Self DeclarationDocument1 pageD Properties Covid 19 Self Declarationfahad atallaNo ratings yet
- Prevention and Treatment of COVID-19 in Elderly People: September 2020Document8 pagesPrevention and Treatment of COVID-19 in Elderly People: September 2020Dra. Adialys Guevara GonzalezNo ratings yet
- Camuso ResumeDocument2 pagesCamuso Resumeapi-548307464No ratings yet
- The Wall Street Journal - 07 04 2020 Optimize PDFDocument34 pagesThe Wall Street Journal - 07 04 2020 Optimize PDFMuhammad HafeezNo ratings yet
- 2.1 DF Non-Thai 7 JulyDocument3 pages2.1 DF Non-Thai 7 JulyJia YapNo ratings yet
- David and Limas EAPS Concept PaperDocument4 pagesDavid and Limas EAPS Concept Paperjepu jepNo ratings yet
- Makalah Bahasa Inggris Unit 6Document10 pagesMakalah Bahasa Inggris Unit 6Nadia NadNo ratings yet
- Letter From The Executive BoardDocument6 pagesLetter From The Executive BoardPratham AryaNo ratings yet
- Rapid Hospital Readiness ChecklistDocument19 pagesRapid Hospital Readiness ChecklistAnonymous KEU60hNo ratings yet
- Tema: Personal Information: Escuela Profesional de EnfermeríaDocument21 pagesTema: Personal Information: Escuela Profesional de EnfermeríaPamela Ballon SotoNo ratings yet
- JP Morgan COVID 19 Presentation PDF PDF PDF PDF PDF PDF PDF PDF PDFDocument45 pagesJP Morgan COVID 19 Presentation PDF PDF PDF PDF PDF PDF PDF PDF PDFFrancoNo ratings yet
- Reflect On The Significant Features of RA 11494.: Treatment of Covid-19 PatientsDocument3 pagesReflect On The Significant Features of RA 11494.: Treatment of Covid-19 PatientsGabriel FranciscoNo ratings yet
- Outpatient Otolaryngology in The Era of COVID-19: A Data-Driven Analysis of Practice PatternsDocument7 pagesOutpatient Otolaryngology in The Era of COVID-19: A Data-Driven Analysis of Practice PatternsMada Dwi HariNo ratings yet