You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Examination of Eye PT IIDocument77 pagesExamination of Eye PT IIMihaela TomaNo ratings yet
- Management of Retinal Detachment: A Guide For Non-OphthalmologistsDocument6 pagesManagement of Retinal Detachment: A Guide For Non-OphthalmologistsadriantiariNo ratings yet
- The Massachusetts Eye Illustrated Manual of Ophthalmology 4th EditionDocument1,212 pagesThe Massachusetts Eye Illustrated Manual of Ophthalmology 4th Editionsare7783% (6)
- Surgical Atlas of Orbital Diseases-Email PDFDocument389 pagesSurgical Atlas of Orbital Diseases-Email PDFAmi Misici100% (1)
- Sample Multiple Choice Questions PDFDocument3 pagesSample Multiple Choice Questions PDFRoseNo ratings yet
- Strabismus: Dr. Digin Mariam OphthalmologyDocument94 pagesStrabismus: Dr. Digin Mariam OphthalmologyVishnu Sai100% (1)
- Ophtha MCQsDocument51 pagesOphtha MCQshenry caze100% (1)
- Ophthalmology MCQsDocument18 pagesOphthalmology MCQsRamachandharan Nethaji67% (9)
- Ophthalmic Manifestation in Langerhans Cell Histio PDFDocument4 pagesOphthalmic Manifestation in Langerhans Cell Histio PDFAmi MisiciNo ratings yet
- CH 8 - Classification of Neuromuscular Anomalies of The Eyes, P. 125-133-EmailDocument8 pagesCH 8 - Classification of Neuromuscular Anomalies of The Eyes, P. 125-133-EmailAmi MisiciNo ratings yet
- CH 9 - Etiology of Heterophoria and Heterotropia, P. 134-152-EmailDocument19 pagesCH 9 - Etiology of Heterophoria and Heterotropia, P. 134-152-EmailAmi MisiciNo ratings yet
- CH 7 - Visual Acuity, Geometric Optical Effects of Spectacles, and Aniseikonia, P. 114-123-EmailDocument10 pagesCH 7 - Visual Acuity, Geometric Optical Effects of Spectacles, and Aniseikonia, P. 114-123-EmailAmi MisiciNo ratings yet
- CH 6 - Histology and Physiology of The Extraocular Muscles, P. 101-113-EmailDocument13 pagesCH 6 - Histology and Physiology of The Extraocular Muscles, P. 101-113-EmailAmi MisiciNo ratings yet
- CH 4 - Physiology of The Ocular Movements, P. 52-84-EmailDocument33 pagesCH 4 - Physiology of The Ocular Movements, P. 52-84-EmailAmi MisiciNo ratings yet
- Cooperation of The EyeDocument5 pagesCooperation of The EyeAmi MisiciNo ratings yet
- GoldenretrieverDocument6 pagesGoldenretrieverTobias-Andreas DietzelNo ratings yet
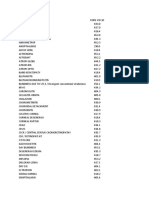
- Kode Icd MataDocument5 pagesKode Icd Mataindah ramadhaniNo ratings yet
- Anisometropia PDFDocument2 pagesAnisometropia PDFIndhumathiNo ratings yet
- Biology Investigatory Project On Eye DiseasesDocument18 pagesBiology Investigatory Project On Eye DiseasesBHALAJI KARUNANITHI100% (1)
- What Is AstigmatismDocument6 pagesWhat Is AstigmatismMernie Grace DionesioNo ratings yet
- 94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Document5 pages94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Catleya ProtacioNo ratings yet
- AbbreviationsDocument2 pagesAbbreviationslovely2886No ratings yet
- EURETINA - Paris19 Final Programme PDFDocument176 pagesEURETINA - Paris19 Final Programme PDFPamela MukhopadhyayNo ratings yet
- Lattice DegenerationDocument3 pagesLattice DegenerationAnumeha JindalNo ratings yet
- Pediatric Glaucoma PDFDocument8 pagesPediatric Glaucoma PDFDr.Nalini PavuluriNo ratings yet
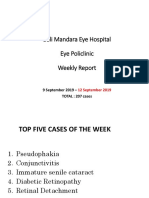
- Bali Mandara Eye Hospital Eye Policlinic Weekly Report: 9 September 2019 - TOTAL: 207 CasesDocument23 pagesBali Mandara Eye Hospital Eye Policlinic Weekly Report: 9 September 2019 - TOTAL: 207 CasesLipo DuoNo ratings yet
- 09 Blindness Prevention Role of Civil Society OrganisationsDocument3 pages09 Blindness Prevention Role of Civil Society OrganisationsMwanja MosesNo ratings yet
- GlaucomaDocument6 pagesGlaucomaCharlie AlmazanNo ratings yet
- Photophobia: Light Sensitivity and Migraines - Webmd: Web ResultsDocument3 pagesPhotophobia: Light Sensitivity and Migraines - Webmd: Web ResultsRheaniesse TreveriaNo ratings yet
- Corneal Dystrophies: Retinal DetachmentDocument6 pagesCorneal Dystrophies: Retinal DetachmentMarissa AsimNo ratings yet
- DR Suman Thapa - Challenges of Glaucome Care in The HimalayasDocument54 pagesDR Suman Thapa - Challenges of Glaucome Care in The HimalayasAn Da100% (1)
- Surgical Management of Dilocated Lens: Mohammad Ghoreishi, MDDocument15 pagesSurgical Management of Dilocated Lens: Mohammad Ghoreishi, MDwawan 88No ratings yet
- The Red Eye Challenge: QuestionsDocument5 pagesThe Red Eye Challenge: QuestionsDaniel CrookNo ratings yet
- Worldwide Distribution of Visual Refractive Error1Document8 pagesWorldwide Distribution of Visual Refractive Error1Rian AprizaNo ratings yet
- DT StrabismusDocument42 pagesDT StrabismushamzahNo ratings yet
- MR 180 EditedDocument6 pagesMR 180 EditedfatmadianaNo ratings yet
- Dr. Med. Reinhard Smettan Dr. Med. Heike Smettan: GemeinschaftspraxisDocument46 pagesDr. Med. Reinhard Smettan Dr. Med. Heike Smettan: GemeinschaftspraxiselrhavNo ratings yet
- Preventive OphthalmologyDocument2 pagesPreventive Ophthalmologysarguss14100% (1)