You might also like
- Behavioral Neurobiology of PTSDDocument274 pagesBehavioral Neurobiology of PTSDCarlos Hernan Castañeda Ruiz100% (1)
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)From EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)No ratings yet
- Vegan Keto For Beginners by Meghan BarnesDocument365 pagesVegan Keto For Beginners by Meghan BarnesDanielaSalinas90% (10)
- Local Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)From EverandLocal Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)No ratings yet
- Inferior Dental Blocks Versus Infiltration DentistryDocument11 pagesInferior Dental Blocks Versus Infiltration DentistryQurrat-ul-AinNo ratings yet
- Case Study Lung Adenocarcinoma PDFDocument43 pagesCase Study Lung Adenocarcinoma PDFFrancis Anthony LoslosoNo ratings yet
- The Use of Traditional Chinese Veterinary Medicine in The Treatment of 5 Cases of Neoplastic Bone DiseaseDocument12 pagesThe Use of Traditional Chinese Veterinary Medicine in The Treatment of 5 Cases of Neoplastic Bone DiseaseDonnaNo ratings yet
- KetofolDocument10 pagesKetofolDr. Shivkumar Kiran AngadiNo ratings yet
- Anesthesia in Endodontics - Facts & Myths PDFDocument6 pagesAnesthesia in Endodontics - Facts & Myths PDFVioleta BotnariNo ratings yet
- Scrabble - Indoor Recreational ActivitiesDocument24 pagesScrabble - Indoor Recreational ActivitiesKimberly TanalasNo ratings yet
- Pharmacology Notes: By: Khurram AbbasDocument48 pagesPharmacology Notes: By: Khurram AbbasAsma AnjumNo ratings yet
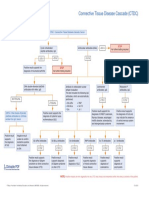
- Connective Tissue Disease CascadeDocument1 pageConnective Tissue Disease CascadeYustina BubnovaNo ratings yet
- HAAD Exam QuestionsDocument7 pagesHAAD Exam QuestionsAsma AnjumNo ratings yet
- Nerve Injury Following A Mandibular BlockDocument7 pagesNerve Injury Following A Mandibular BlockKranti PrajapatiNo ratings yet
- Anesthesia Onset Time and Injection Pain Between Buffered and Unbuffered Lidocaine Used As Local Anesthetic For Dental Care in ChildrenDocument4 pagesAnesthesia Onset Time and Injection Pain Between Buffered and Unbuffered Lidocaine Used As Local Anesthetic For Dental Care in ChildrenFernando MenesesNo ratings yet
- Os 2Document4 pagesOs 2مرتضى محمد فاضل جرجوكNo ratings yet
- Conscious Sedation in Pediatric Dentistry A ReviewDocument4 pagesConscious Sedation in Pediatric Dentistry A Reviewjyothi shashidharNo ratings yet
- MirasolDocument7 pagesMirasolJan Chrispian MirasolNo ratings yet
- 9384 - Original ResearchDocument3 pages9384 - Original ResearchAnita PrastiwiNo ratings yet
- Toxicidad Anestesicos LocalesDocument11 pagesToxicidad Anestesicos LocalesCamilo MoraNo ratings yet
- Local and Regional Anaesthesia in Dogs Cats Part 1 Overview of Concepts Drugs Grubb Lobprise 2020Document9 pagesLocal and Regional Anaesthesia in Dogs Cats Part 1 Overview of Concepts Drugs Grubb Lobprise 2020Carolina Duque RodriguezNo ratings yet
- Paul Hobeich, DMD, Stephen Simon, DMD, Emit Schneiderman, PHD, and Jianing He, DMD, PHDDocument3 pagesPaul Hobeich, DMD, Stephen Simon, DMD, Emit Schneiderman, PHD, and Jianing He, DMD, PHDDaniella NúñezNo ratings yet
- Kulkarni 2019Document13 pagesKulkarni 2019Byron ChávezNo ratings yet
- The Use of Hypnosis and Systematic Desensitisation in The Management of Dental Phobia A Case ReportDocument6 pagesThe Use of Hypnosis and Systematic Desensitisation in The Management of Dental Phobia A Case ReportAnissa Citra UtamiNo ratings yet
- General Anesthesia Thesis TopicsDocument7 pagesGeneral Anesthesia Thesis Topicsandreachristianreno100% (2)
- Sustained-Release Lidocaine Sheet For Pain FollowiDocument19 pagesSustained-Release Lidocaine Sheet For Pain FollowiArianny PerazaNo ratings yet
- Premed ConsiderationDocument9 pagesPremed Considerationaditya brahmantio sujakaNo ratings yet
- 2 GeneralDocument9 pages2 GeneralajenggayatriNo ratings yet
- Desflurane Versus Sevoflurane For Maintenance Of.17Document7 pagesDesflurane Versus Sevoflurane For Maintenance Of.17AndresPimentelAlvarezNo ratings yet
- Commerce: Research Paper Role of Conscious Sedation in DentistryDocument2 pagesCommerce: Research Paper Role of Conscious Sedation in DentistryDiamanta Yalomit CirsteaNo ratings yet
- Recent Advances in LA - JCDocument6 pagesRecent Advances in LA - JCraghurvp109No ratings yet
- 2012 Nourbakhsh Effect of Phentolamine Mesylate On Duration of Soft Tissue Local Anesthesia in ChildrenDocument8 pages2012 Nourbakhsh Effect of Phentolamine Mesylate On Duration of Soft Tissue Local Anesthesia in ChildrenBryant LewisNo ratings yet
- Perineural Adjuncts For Peripheral Nerve BlockDocument7 pagesPerineural Adjuncts For Peripheral Nerve BlockpitriaNo ratings yet
- Anxiolysis in Dental Practice - A Report of Three CasesDocument7 pagesAnxiolysis in Dental Practice - A Report of Three CasesAnaMariaCastroNo ratings yet
- Anesthetic Drugs Jonathan Bland Pathophysiology Professor Lori McgowanDocument4 pagesAnesthetic Drugs Jonathan Bland Pathophysiology Professor Lori McgowanjonNo ratings yet
- Maxillary Lateral Incisor Injection Pain Using The Dentapen Electronic SyringeDocument5 pagesMaxillary Lateral Incisor Injection Pain Using The Dentapen Electronic SyringeKEY 1111No ratings yet
- EpinephrineDocument5 pagesEpinephrinesheynnaNo ratings yet
- Analgesia y Anestesia Oral en Perro y Gato VCSADocument18 pagesAnalgesia y Anestesia Oral en Perro y Gato VCSAValentina AmayaNo ratings yet
- South Erland 2016Document38 pagesSouth Erland 2016jennyfilgueira001No ratings yet
- Use of Local Anesthesia For Pediatric DentalDocument6 pagesUse of Local Anesthesia For Pediatric DentalمعتزباللهNo ratings yet
- Practice Guidelines For Sedation and Analgesia by Non-AnesthesiologistsDocument14 pagesPractice Guidelines For Sedation and Analgesia by Non-AnesthesiologistsNurbani 28nersNo ratings yet
- Ijca 7 2 313 318Document6 pagesIjca 7 2 313 318Bianca CaterinalisendraNo ratings yet
- Scientific Dental JournalDocument4 pagesScientific Dental JournalMutia KumalasariNo ratings yet
- Guia Asa de Anestesia General y SedaciónDocument43 pagesGuia Asa de Anestesia General y SedaciónAlfonso Antioco Gonzalez RojasNo ratings yet
- 3 LRA 10237 Epidural Analgesia For Labor 120710Document11 pages3 LRA 10237 Epidural Analgesia For Labor 120710Nur Rissa MaharanyNo ratings yet
- The Effects of Listening To The Qur'an in The Postoperative Management ofDocument5 pagesThe Effects of Listening To The Qur'an in The Postoperative Management ofdindaikaputriNo ratings yet
- MalamedDocument7 pagesMalamedProgynanika BarmanNo ratings yet
- Oral Clonidine Pre-Treatment and Diazepam/Meperidine SedationDocument5 pagesOral Clonidine Pre-Treatment and Diazepam/Meperidine Sedationmapecorelli2626No ratings yet
- The Routes of Administration For Acute Postoperative Pain MedicationDocument17 pagesThe Routes of Administration For Acute Postoperative Pain Medicationronald97hgNo ratings yet
- Conscious SedationDocument55 pagesConscious Sedationankita rajNo ratings yet
- Analgesia Multimodal en Cirugía AmbulatoriaDocument7 pagesAnalgesia Multimodal en Cirugía AmbulatoriaChurrunchaNo ratings yet
- Anestesia 1Document22 pagesAnestesia 1Carlos MNo ratings yet
- Snyder 2016Document7 pagesSnyder 2016Arturo TrujilloNo ratings yet
- Pharmacologic Management of Adult Breakthrough Cancer Pain: Palliative Care FilesDocument4 pagesPharmacologic Management of Adult Breakthrough Cancer Pain: Palliative Care Filesousama aklan100% (1)
- Dexamethasone: Continuing EducationDocument5 pagesDexamethasone: Continuing EducationTina PatelNo ratings yet
- A Comparison of Periodontal Intraligamental Anesthesia Using Etidocaine HCI and Lidocaine HCIDocument4 pagesA Comparison of Periodontal Intraligamental Anesthesia Using Etidocaine HCI and Lidocaine HCITeremfMoraNo ratings yet
- Sudhakar 2014 The Efficacy of Different Pre and Post Operative Analgesics in The Management of Pain After Orthodontic Separator PlacementDocument6 pagesSudhakar 2014 The Efficacy of Different Pre and Post Operative Analgesics in The Management of Pain After Orthodontic Separator PlacementTarif HamshoNo ratings yet
- Local Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryDocument8 pagesLocal Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryFrancisco Javier Rodriguez MolinaNo ratings yet
- Nihms-1579274 PDFDocument23 pagesNihms-1579274 PDFAhmed ElshewiNo ratings yet
- Anestietics: DentstyDocument8 pagesAnestietics: Dentstyblabarry1109No ratings yet
- Local Anesthesia Drugs CDA 2006 MalamedDocument6 pagesLocal Anesthesia Drugs CDA 2006 MalamedSaj1985100% (2)
- MalamedDocument8 pagesMalamedDr. DhDhNo ratings yet
- Local Anaesthesia in Dentistry A ReviewDocument9 pagesLocal Anaesthesia in Dentistry A ReviewAshyana SaeedNo ratings yet
- 10 PDFDocument8 pages10 PDFSean AndersonNo ratings yet
- 8a. General AnaesthesiaDocument28 pages8a. General Anaesthesiamatchees-gone rogueNo ratings yet
- Articaine Vs LignoncaineDocument8 pagesArticaine Vs Lignoncaineisha MehtaNo ratings yet
- Efficacy of Dental Local Anesthetics A ReviewDocument14 pagesEfficacy of Dental Local Anesthetics A ReviewAlaghen VespanathanNo ratings yet
- 6 Amelogenesis, Dentinogenesis and Root FormationDocument4 pages6 Amelogenesis, Dentinogenesis and Root FormationAsma AnjumNo ratings yet
- A) Immediate Use of Post Immediately After RCT Has Resulted in Decrease Apical LeakageDocument6 pagesA) Immediate Use of Post Immediately After RCT Has Resulted in Decrease Apical LeakageAsma AnjumNo ratings yet
- HAAD Exam 28 April 2012Document3 pagesHAAD Exam 28 April 2012Asma AnjumNo ratings yet
- Perio Recent AdvancesDocument5 pagesPerio Recent AdvancesAsma AnjumNo ratings yet
- Alternative System For Periodontitis Classification Based On The Genetic Signature of Affected Tissue Mar 27, 2014 Columbia University Medical CentreDocument3 pagesAlternative System For Periodontitis Classification Based On The Genetic Signature of Affected Tissue Mar 27, 2014 Columbia University Medical CentreAsma AnjumNo ratings yet
- Professional Skills For ManagersDocument53 pagesProfessional Skills For ManagersAsma AnjumNo ratings yet
- Chronic Venous Disorders New TemplateDocument43 pagesChronic Venous Disorders New TemplateamrNo ratings yet
- Diagnostic Test in Mapeh 6 Name: - Date: - Teacher: - SectionDocument5 pagesDiagnostic Test in Mapeh 6 Name: - Date: - Teacher: - SectionMelanie Joan Abao PaconNo ratings yet
- MainDocument9 pagesMainZahraNo ratings yet
- Revista de Medicină Legală Romanian Journal of Legal Medicine, Vol 19, Issue 3, September 2011Document76 pagesRevista de Medicină Legală Romanian Journal of Legal Medicine, Vol 19, Issue 3, September 2011Diaconita IuliaNo ratings yet
- Meconium Aspiration SyndromeDocument20 pagesMeconium Aspiration SyndromeLevi PosadasNo ratings yet
- Mari 2006Document4 pagesMari 2006Nico NicoNo ratings yet
- Katarak Pada Anak PerdamiDocument9 pagesKatarak Pada Anak PerdamiMahendra M NurmawanNo ratings yet
- What Are The Pros and Cons of MarijuanaDocument10 pagesWhat Are The Pros and Cons of Marijuanaapi-550020088No ratings yet
- Case 10 Shutter IslandDocument3 pagesCase 10 Shutter IslandAnkith ReddyNo ratings yet
- ĐIỀN TỪ VÀO ĐOẠN VĂN - ANH 9Document5 pagesĐIỀN TỪ VÀO ĐOẠN VĂN - ANH 9nvo169007No ratings yet
- Pancreatic Pseudocyst EDITEDDocument5 pagesPancreatic Pseudocyst EDITEDLaura LatifaNo ratings yet
- Winter Here New Title.Document184 pagesWinter Here New Title.Christopher VecchittoNo ratings yet
- Metalodrogas y Química InorgánicaDocument24 pagesMetalodrogas y Química InorgánicaCristhian D EchevesteNo ratings yet
- Syllabus Group - C & DDocument87 pagesSyllabus Group - C & DAnupam DhawaleNo ratings yet
- Facts MainDocument3 pagesFacts MainSAI CHAITANYA YEPURINo ratings yet
- Biochem Term PaperDocument5 pagesBiochem Term PaperVincent Philip DelavictoriaNo ratings yet
- Hospital Thesis ArchitectureDocument8 pagesHospital Thesis Architecturefbyhhh5r100% (2)
- How Can I Protect Myself and Others?: COVID-19!Document39 pagesHow Can I Protect Myself and Others?: COVID-19!Stefan MilutinovićNo ratings yet
- Field ParasitologyDocument73 pagesField ParasitologyMALIK WASEEM ABBASNo ratings yet
- Sib 3 HW 3 15Document5 pagesSib 3 HW 3 15joud.dekayelNo ratings yet
- New Test of Competence Webinar Slides 3 December 2020Document42 pagesNew Test of Competence Webinar Slides 3 December 2020Donald QuackNo ratings yet
- Chapter 2 - Review of Related Literature Group1 - Humss11 D 4Document20 pagesChapter 2 - Review of Related Literature Group1 - Humss11 D 4Paul Francis LagmanNo ratings yet
- Goals, Target & Indicator of 2030 Sustainable Development GoalsDocument56 pagesGoals, Target & Indicator of 2030 Sustainable Development GoalsSkawn GurNo ratings yet
- EHTPA CurriculumDocument109 pagesEHTPA Curriculumjle_dl0% (1)