You might also like
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- 2018 - Banyak Foto - Oral Rehabilitation of The Cancer PatientDocument18 pages2018 - Banyak Foto - Oral Rehabilitation of The Cancer PatientSyifa IKNo ratings yet
- Periodontal Considerations in The Management of The Cancer PatientDocument11 pagesPeriodontal Considerations in The Management of The Cancer PatientGilda Delgado MonsalveNo ratings yet
- Requirement and Responsibility MFPDocument4 pagesRequirement and Responsibility MFPAlexandru Codrin-IonutNo ratings yet
- Iis ManisDocument6 pagesIis ManisNurbaetty RochmahNo ratings yet
- Chen 2019Document9 pagesChen 2019Tiara HapkaNo ratings yet
- 26 - 2 - 193 - Oral Surgery in Patients Undergoing Chemoradiation Therapy PDFDocument15 pages26 - 2 - 193 - Oral Surgery in Patients Undergoing Chemoradiation Therapy PDFTabishur RahmanNo ratings yet
- Oral Surgery in Patients Undergoing Chemoradiation TherapyDocument15 pagesOral Surgery in Patients Undergoing Chemoradiation TherapyTabishur RahmanNo ratings yet
- Article 1459955174Document9 pagesArticle 1459955174Nia LieantoNo ratings yet
- Rehabilitation Following Partion Glossectomy and Neck DissectionDocument10 pagesRehabilitation Following Partion Glossectomy and Neck DissectionnotmelbrooksNo ratings yet
- Prosthodontic Rehabilitation ofDocument23 pagesProsthodontic Rehabilitation ofDaniel PozzosNo ratings yet
- ObturatorDocument7 pagesObturatordrgayen6042No ratings yet
- Orthognathic Surgery Versus Orthodontic Camouflage in The Treatment of Mandibular DeficiencyDocument7 pagesOrthognathic Surgery Versus Orthodontic Camouflage in The Treatment of Mandibular DeficiencyDiana ElíasNo ratings yet
- Risk Factors in Bone Augmentation Procedures: Peter K. Moy - Tara AghalooDocument15 pagesRisk Factors in Bone Augmentation Procedures: Peter K. Moy - Tara Aghalooxiaoxin zhangNo ratings yet
- Oral Oncology: SciencedirectDocument10 pagesOral Oncology: SciencedirectLisbeth TurraNo ratings yet
- Peri ImplantitisDocument12 pagesPeri ImplantitisbobNo ratings yet
- Over Sem EsplintarDocument9 pagesOver Sem EsplintarClaudia BrilhanteNo ratings yet
- Full Mouth RehabDocument37 pagesFull Mouth RehabAravind Krishnan100% (4)
- Regenerative Endodontics Barriers and Strategies For Clinical Translation 2012 Dental Clinics of North AmericaDocument11 pagesRegenerative Endodontics Barriers and Strategies For Clinical Translation 2012 Dental Clinics of North AmericaCaioSelaimenNo ratings yet
- Classification of Tongue Cancer Resection and Treatment AlgorithmDocument8 pagesClassification of Tongue Cancer Resection and Treatment AlgorithmRahma WatiNo ratings yet
- Palliative Dental 2014Document6 pagesPalliative Dental 2014Isteicy CortezNo ratings yet
- Management of Oral Cancer (1) ...Document3 pagesManagement of Oral Cancer (1) ...Mircea IlieNo ratings yet
- Root Resorption A 6-Year Follow-Up Case ReportDocument3 pagesRoot Resorption A 6-Year Follow-Up Case Reportpaola lopezNo ratings yet
- Orthodontic Management of Patients With Cleft Lip and Palate PDFDocument6 pagesOrthodontic Management of Patients With Cleft Lip and Palate PDFcareNo ratings yet
- Prosthetic Rehabilitation of Acquired Maxillofacial Defect Obturating Residual Oronasal Communication A Clinical Report 91 93Document3 pagesProsthetic Rehabilitation of Acquired Maxillofacial Defect Obturating Residual Oronasal Communication A Clinical Report 91 93Maqbul AlamNo ratings yet
- Jurnal CRSS Prothesa 4 (Sixna Agitha Claresta 20204020100)Document7 pagesJurnal CRSS Prothesa 4 (Sixna Agitha Claresta 20204020100)sixnaagithaNo ratings yet
- PMF 1Document4 pagesPMF 1Andrei CrețuNo ratings yet
- 19 FullDocument5 pages19 FullBramita Beta ArnandaNo ratings yet
- Full Mouth Fixed Implant Rehabilitation in A Patient With Generalized Aggressive PeriodontitisDocument6 pagesFull Mouth Fixed Implant Rehabilitation in A Patient With Generalized Aggressive PeriodontitisFernando CursachNo ratings yet
- Guia de Tratamiento PeriodontalDocument6 pagesGuia de Tratamiento PeriodontalSam PicturNo ratings yet
- Dentistry 12 00083Document13 pagesDentistry 12 00083adiNo ratings yet
- Carranza's Clinical Periodontology 2002Document6 pagesCarranza's Clinical Periodontology 2002Lia Optimeze Alwayz100% (1)
- Hickey 1991Document6 pagesHickey 1991Hema SinghNo ratings yet
- E PerioTherapyDocument5 pagesE PerioTherapymaherinoNo ratings yet
- 39 UyifDocument12 pages39 UyifGeorgia.annaNo ratings yet
- Maxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. HaugDocument11 pagesMaxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. Hauglaura sanchez avilaNo ratings yet
- Dental Problems in Pediatric Patients With Head and Neck Tumors Undergoing Multiple Modality TherapyDocument5 pagesDental Problems in Pediatric Patients With Head and Neck Tumors Undergoing Multiple Modality Therapyمحمد عبدالرحمنNo ratings yet
- Kumar2019 230312 014011Document5 pagesKumar2019 230312 014011navyaNo ratings yet
- Parameters of Care Supplement: Parameter On Occlusal Traumatism in Patients With Chronic PeriodontitisDocument3 pagesParameters of Care Supplement: Parameter On Occlusal Traumatism in Patients With Chronic PeriodontitisSeema ShekhawatNo ratings yet
- Case Report Multidisciplinary Oral Rehabilitation of A Severely Compromised DentitionDocument7 pagesCase Report Multidisciplinary Oral Rehabilitation of A Severely Compromised DentitionAgum Nila Sari IINo ratings yet
- Sclar 2004Document16 pagesSclar 2004Kelly N100% (1)
- Premium Day Poster COIR 2013Document28 pagesPremium Day Poster COIR 2013juanNo ratings yet
- Cap 5Document22 pagesCap 5Elena DimitriuNo ratings yet
- READINGDocument11 pagesREADINGThea DuoNo ratings yet
- Oral Sugery in Medically Compromised PatientDocument11 pagesOral Sugery in Medically Compromised PatientDrdilip PathakNo ratings yet
- Treatment Trends in PeriodonticsDocument8 pagesTreatment Trends in Periodonticspatricia sotoNo ratings yet
- Todentj 11 581Document14 pagesTodentj 11 581gifar ihsanNo ratings yet
- 2006 4 Oral - Cancer PDFDocument225 pages2006 4 Oral - Cancer PDFAnonymous ENwjWryNo ratings yet
- Prosthodontic Rehabilitation of Patient With Anterior HyperDocument5 pagesProsthodontic Rehabilitation of Patient With Anterior HyperGin Gin GustianaNo ratings yet
- Provisional Prosthesis For Class 1 Radical Mandibular Alveolectomy Patient - A Case ReportDocument5 pagesProvisional Prosthesis For Class 1 Radical Mandibular Alveolectomy Patient - A Case ReportRastia UtamiNo ratings yet
- Mds - Curriculum (Hust) Tongji Medical CollegeDocument45 pagesMds - Curriculum (Hust) Tongji Medical CollegeMukunda RegmiNo ratings yet
- Three Different Surgical Techniques of Crown Lengthening: A Comparative StudyDocument10 pagesThree Different Surgical Techniques of Crown Lengthening: A Comparative StudyWiet SidhartaNo ratings yet
- Uribe Et Al. 2019. Surgery-First Approach inDocument15 pagesUribe Et Al. 2019. Surgery-First Approach inAlvaro jose Uribe TamaraNo ratings yet
- Sefalo 3Document6 pagesSefalo 3Aisha DewiNo ratings yet
- Chandu 2002Document4 pagesChandu 2002Guma KipaNo ratings yet
- Orthognathic Surgery Correction of Dentofacial DeformitiesDocument14 pagesOrthognathic Surgery Correction of Dentofacial Deformitiesmarina.huppiNo ratings yet
- MesializationDocument7 pagesMesializationTesisTraduccionesRuzelNo ratings yet
- IndianJPalliatCare DentistaDocument5 pagesIndianJPalliatCare DentistaIsteicy CortezNo ratings yet
- The Pathology of Melanoma:: An International CourseDocument4 pagesThe Pathology of Melanoma:: An International CourseElena BadiuNo ratings yet
- 8th Emirates Pathology & Digital Pathology Conference Program - T 10-12, 2021 OnlineDocument14 pages8th Emirates Pathology & Digital Pathology Conference Program - T 10-12, 2021 OnlineElena BadiuNo ratings yet
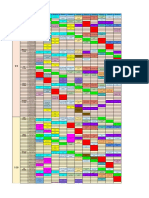
- Data/zi Grupa 1 Grupa 2 Grupa 3 Grupa 4 Grupa 5 Grupa 6 Grupa 7 Grupa 8 Grupa 9 Grupa 10 Grupa 11 Luni 12-AprDocument4 pagesData/zi Grupa 1 Grupa 2 Grupa 3 Grupa 4 Grupa 5 Grupa 6 Grupa 7 Grupa 8 Grupa 9 Grupa 10 Grupa 11 Luni 12-AprElena BadiuNo ratings yet
- Niculet 4 18Document4 pagesNiculet 4 18Elena BadiuNo ratings yet
- How To Teach Pathology To Medical Students: Bharti and Shivayogi Bhusnurmath ST Georges University, Grenada, West IndiesDocument60 pagesHow To Teach Pathology To Medical Students: Bharti and Shivayogi Bhusnurmath ST Georges University, Grenada, West IndiesElena BadiuNo ratings yet
- Artifacts in Hematology by Dr. Bakul DalalDocument11 pagesArtifacts in Hematology by Dr. Bakul DalalDr MayurNo ratings yet
- Lecciones Basicas en Control de Calidad.2008 Bio-Rad InglesDocument62 pagesLecciones Basicas en Control de Calidad.2008 Bio-Rad InglesPili Gabriel67% (3)
- Bacterial Contamination of BlenderizedDocument23 pagesBacterial Contamination of BlenderizedAgnes Alulod BuenaaguaNo ratings yet
- Special Pathology Viva Questions by AMS 46Document32 pagesSpecial Pathology Viva Questions by AMS 46Mohan Dass100% (1)
- Zhang2020 Article EvaluationOfBepanGelHydrogelEfDocument14 pagesZhang2020 Article EvaluationOfBepanGelHydrogelEfİncelus ChinusNo ratings yet
- Psychoneuroimmunology Anu Final 1 1Document30 pagesPsychoneuroimmunology Anu Final 1 1Haris AhmedNo ratings yet
- Biomedical Waste Management Colour Coding For BeginnersDocument3 pagesBiomedical Waste Management Colour Coding For BeginnersMotherterrasa VocationalNo ratings yet
- What Is The Difference Between Tendonitis, Tendinosis, and TendinopathyDocument3 pagesWhat Is The Difference Between Tendonitis, Tendinosis, and TendinopathySylvia GraceNo ratings yet
- DuchenneDocument13 pagesDuchennejenika studiesNo ratings yet
- Urinary Tract I-WPS OfficeDocument21 pagesUrinary Tract I-WPS Officekersameeksha borkerNo ratings yet
- Medication - Chart ADHD PDFDocument2 pagesMedication - Chart ADHD PDFaayceeNo ratings yet
- Acupuntura - Puntos ImportantesDocument14 pagesAcupuntura - Puntos ImportantessanthigiNo ratings yet
- Tibetan Medicine and The CoronavirusDocument1 pageTibetan Medicine and The CoronavirusIvan IvanicNo ratings yet
- If The Physician Diagnoses The Patient Wrongly He Would Get BeatenDocument4 pagesIf The Physician Diagnoses The Patient Wrongly He Would Get BeatenSheen GabatoNo ratings yet
- Daftar Sampel ReadyDocument6 pagesDaftar Sampel ReadydindaNo ratings yet
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- New Insulin Delivery Recommendations: Supplemental Ap-Pendix 1Document25 pagesNew Insulin Delivery Recommendations: Supplemental Ap-Pendix 1Fariza AyudiaNo ratings yet
- Ocular Features in A Large Cohort of Indians With.5Document7 pagesOcular Features in A Large Cohort of Indians With.5Sushma NNo ratings yet
- Is Lipedema A Unique Entity?Document7 pagesIs Lipedema A Unique Entity?Alexandre Campos Moraes AmatoNo ratings yet
- Inpatient Glycemic ManagementDocument13 pagesInpatient Glycemic Managementmiss betawiNo ratings yet
- Allergic Rhinitis in ChildrenDocument7 pagesAllergic Rhinitis in ChildrenTina MorleyNo ratings yet
- Core Knowledge OrthopaedicsDocument2 pagesCore Knowledge OrthopaedicsIamTineshNo ratings yet
- Guideline of Urolithiasis PDFDocument34 pagesGuideline of Urolithiasis PDFMelia IndasariNo ratings yet
- D-Patient Verbalized "Sakit Gyod Akong Tiyan", Pain: Sample 1Document29 pagesD-Patient Verbalized "Sakit Gyod Akong Tiyan", Pain: Sample 1jaypee100% (3)
- pedCAT BrochureDocument12 pagespedCAT BrochureVinti Singh100% (1)
- What It Takes To Be A Doctor?Document11 pagesWhat It Takes To Be A Doctor?Marion YaoNo ratings yet
- Prostatitis: Symptoms, Causes and TreatmentsDocument16 pagesProstatitis: Symptoms, Causes and TreatmentsjoserodrrNo ratings yet
- CS - UTI, Acute Bronchitis, Acute GastritisDocument39 pagesCS - UTI, Acute Bronchitis, Acute GastritisGrace BernadetteNo ratings yet
- A Three-Dimensional Method of Visualizing The Temporomandibular Joint Based On Magnetic Resonance Imaging in A Case of Juvenile Chronic ArthritisDocument7 pagesA Three-Dimensional Method of Visualizing The Temporomandibular Joint Based On Magnetic Resonance Imaging in A Case of Juvenile Chronic ArthritisNAGARAJNo ratings yet
- Foundations Adult Health Nursing 8th Cooper Test BankDocument15 pagesFoundations Adult Health Nursing 8th Cooper Test BankRaadqqqNo ratings yet
- Hcs Customer BrochureDocument43 pagesHcs Customer BrochureKunalNo ratings yet
- Diane Kazer Loving On Our LymphDocument22 pagesDiane Kazer Loving On Our LymphKátia BárbaraNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)