You might also like
- Distal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDistal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Exercises for Patella (Kneecap) Pain, Patellar Tendinitis, and Common Operations for Kneecap Problems: - Understanding kneecap problems and patellar tendinitis - Conservative rehabilitation protocols - Rehabilitation protocols for lateral release, patellar realignment, medial patellofemoral ligament reFrom EverandExercises for Patella (Kneecap) Pain, Patellar Tendinitis, and Common Operations for Kneecap Problems: - Understanding kneecap problems and patellar tendinitis - Conservative rehabilitation protocols - Rehabilitation protocols for lateral release, patellar realignment, medial patellofemoral ligament reRating: 5 out of 5 stars5/5 (1)
- Total Knee Replacement (TKR) : Dr. Aamer NaeemDocument41 pagesTotal Knee Replacement (TKR) : Dr. Aamer NaeemfaizasaleemsameNo ratings yet
- Knee Osteoarthritis: DefinitionDocument19 pagesKnee Osteoarthritis: DefinitionShrouq BadrNo ratings yet
- Oa KneeDocument17 pagesOa KneeChitra ChauhanNo ratings yet
- Cinahl Rotator Cuff InjuriesDocument11 pagesCinahl Rotator Cuff InjurieslizardbeeNo ratings yet
- Total Knee ArthroplastyDocument16 pagesTotal Knee Arthroplastyapi-668800855No ratings yet
- The Hip: Therapeutic Exercise 2 Lino Linford BangayanDocument91 pagesThe Hip: Therapeutic Exercise 2 Lino Linford BangayanLino Linford Yu Bangayan100% (1)
- OsteoarthritisDocument45 pagesOsteoarthritisMar ClrNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- REVISION TKR DR Hamad DammamDocument108 pagesREVISION TKR DR Hamad DammamFahad MNo ratings yet
- Q&A About Total Knee ReplacementDocument4 pagesQ&A About Total Knee ReplacementDrManoj JagarlamudiNo ratings yet
- Arthritis (Cabansag, Ma. Flor-And-Cabansag, Joyce)Document38 pagesArthritis (Cabansag, Ma. Flor-And-Cabansag, Joyce)Carlojay IniegoNo ratings yet
- Knee OsteoarthritisDocument3 pagesKnee OsteoarthritispandukajayakuruNo ratings yet
- Degenerative Disorders of JointsDocument25 pagesDegenerative Disorders of JointsayuNo ratings yet
- TKRDocument11 pagesTKRbajay1234No ratings yet
- Knee OsteoarthritisDocument22 pagesKnee OsteoarthritisHK FreeNo ratings yet
- Principle of Fracture & Dislocation ManagementDocument118 pagesPrinciple of Fracture & Dislocation ManagementBryan LeongNo ratings yet
- Talar Fracture Repair and RehabilitationDocument4 pagesTalar Fracture Repair and RehabilitationAlexandra NadinneNo ratings yet
- Lumbar Laminectomy Surgery For Spinal StenosisDocument15 pagesLumbar Laminectomy Surgery For Spinal StenosisElizabeth Liles MartinezNo ratings yet
- Anatomy 3Document52 pagesAnatomy 3Balsam TeineNo ratings yet
- Osteoarthritis Clinical Pattern Sheet PDFDocument5 pagesOsteoarthritis Clinical Pattern Sheet PDFWaseem Khan AfridiNo ratings yet
- Osteoarthritis: By: Vien HardiyantiDocument37 pagesOsteoarthritis: By: Vien HardiyantiPhannyta CherryNo ratings yet
- Orthopedics Standard of Care GuidelinesDocument543 pagesOrthopedics Standard of Care GuidelinesppeterarmstrongNo ratings yet
- Femur Leg FracturesDocument78 pagesFemur Leg FracturesAnonymous hTivgzixVNNo ratings yet
- نسخة light blue creative modern medical clinic presentationDocument33 pagesنسخة light blue creative modern medical clinic presentationFaresNo ratings yet
- 2 2-ArthritidesDocument76 pages2 2-ArthritidesAvinash KaushikNo ratings yet
- Ankle SprainsDocument18 pagesAnkle Sprainsnelson1313No ratings yet
- Caring For Patients With Musculoskeletal DisordersDocument16 pagesCaring For Patients With Musculoskeletal DisorderszebeneNo ratings yet
- Osteoarthritis: Dr. C. C. VisserDocument85 pagesOsteoarthritis: Dr. C. C. VisserAhmad Fathira FitraNo ratings yet
- Acl Rupturer - TextbookDocument26 pagesAcl Rupturer - TextbookFakhrun Nisa WitringNo ratings yet
- Ra and Osteoarthritis R IfDocument43 pagesRa and Osteoarthritis R IfsnfhanNo ratings yet
- NCM 104 MusculoskeletalDocument12 pagesNCM 104 MusculoskeletalCJ AngelesNo ratings yet
- Accessory Navicular BoneDocument29 pagesAccessory Navicular BonePhysiotherapist AliNo ratings yet
- Protocol AchillesTendinosisDocument11 pagesProtocol AchillesTendinosisPhooi Yee LauNo ratings yet
- 02.elbow PainDocument62 pages02.elbow PainKhushboo IkramNo ratings yet
- Student Handbook 11-1Document40 pagesStudent Handbook 11-1archmagus2345No ratings yet
- Sports Injuries in UE - Shoulder - Part 3.Document87 pagesSports Injuries in UE - Shoulder - Part 3.salmankhan09215No ratings yet
- Management of Knee OsteoarthritisDocument35 pagesManagement of Knee OsteoarthritisChukwuemeka ChidogoNo ratings yet
- What Is Spinal StenosisDocument10 pagesWhat Is Spinal Stenosismariamel31No ratings yet
- Ankle D.DDocument16 pagesAnkle D.Dمحمد عقلNo ratings yet
- Knee Injuries: DR - Sindhu Meena MEM Resident MMHRCDocument30 pagesKnee Injuries: DR - Sindhu Meena MEM Resident MMHRCP Vinod KumarNo ratings yet
- Patellar Tendon RuptureDocument13 pagesPatellar Tendon Rupturededyalkarni08No ratings yet
- Knee Pain and ProblemsDocument3 pagesKnee Pain and ProblemsAnshu AgarwalNo ratings yet
- Degenerative Joint Diseases - Admisson ExamDocument23 pagesDegenerative Joint Diseases - Admisson ExamNona NadimNo ratings yet
- Spinal SurgeryDocument19 pagesSpinal SurgerySalomeSibashviliNo ratings yet
- Osteoarthritis 191016103144Document49 pagesOsteoarthritis 191016103144dr.abouzaid098No ratings yet
- Chapter-7-Orthopedic EmergenciesDocument24 pagesChapter-7-Orthopedic EmergenciesALAY DRUSSNo ratings yet
- Tuberculosis of Hip JointDocument25 pagesTuberculosis of Hip JointYousra ShaikhNo ratings yet
- Ligament Injury Around KneeDocument96 pagesLigament Injury Around KneeIvan Olo SarumpaetNo ratings yet
- 13 - Musculoskeletal System AssessmentDocument53 pages13 - Musculoskeletal System Assessmente.mb275No ratings yet
- TKRA-up To DateDocument52 pagesTKRA-up To DateDerek Ho Jong RaNo ratings yet
- Long Bone Fracture Management - Dr. ImanDocument20 pagesLong Bone Fracture Management - Dr. ImanYuliusNo ratings yet
- OsteoarthritisDocument39 pagesOsteoarthritisRohit RajeevNo ratings yet
- Avascular NecrosisDocument49 pagesAvascular NecrosisvhugalabudeliNo ratings yet
- Management of Patellofemoral Chondral InjuriesDocument24 pagesManagement of Patellofemoral Chondral InjuriesBenalNo ratings yet
- Surgery Ortho - TaskDocument4 pagesSurgery Ortho - TasknicewanNo ratings yet
- Osteoarthritis of HipDocument3 pagesOsteoarthritis of Hipjcachica21No ratings yet
- Self Assessment in Musculoskeletal Pathology X-raysFrom EverandSelf Assessment in Musculoskeletal Pathology X-raysRating: 5 out of 5 stars5/5 (2)
- Category 3 Week 8Document1 pageCategory 3 Week 8api-468093714No ratings yet
- Week 8 Category 2Document4 pagesWeek 8 Category 2api-468093714No ratings yet
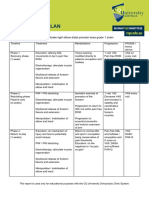
- Zac Williams Simple MSK Management PlanDocument1 pageZac Williams Simple MSK Management Planapi-468093714No ratings yet
- Week 5 Category 2 QuestionsDocument4 pagesWeek 5 Category 2 Questionsapi-468093714No ratings yet
- Week 7 Category 3Document3 pagesWeek 7 Category 3api-468093714No ratings yet
- Group 1 Tutorial IcaDocument7 pagesGroup 1 Tutorial Icaapi-468093714No ratings yet
- cp120 Competency ListDocument1 pagecp120 Competency Listapi-468093714No ratings yet
- Fms Score SheetDocument2 pagesFms Score Sheetapi-468093714No ratings yet
- Management Plan 1Document6 pagesManagement Plan 1api-468093714No ratings yet
- Oswestry Disability Index Odi Editable 1Document2 pagesOswestry Disability Index Odi Editable 1api-468093714No ratings yet
- DRUG STUDY Ft. RanitidineDocument4 pagesDRUG STUDY Ft. RanitidinePao LaurenteNo ratings yet
- Gall Stone CleanseDocument11 pagesGall Stone CleanseLoyiso GumaNo ratings yet
- Mihal V Mcmaster - Complaint - 4-5-21Document21 pagesMihal V Mcmaster - Complaint - 4-5-21WMBF News100% (1)
- Quarter 2 - Module 4 - Earth and Life ScienceDocument5 pagesQuarter 2 - Module 4 - Earth and Life ScienceKristine AlcordoNo ratings yet
- Microbiology Course FileDocument41 pagesMicrobiology Course FileRavi IndraNo ratings yet
- Immediate DenturesDocument35 pagesImmediate DenturesPrince AhmedNo ratings yet
- E&M SheetDocument4 pagesE&M SheettimvrghsNo ratings yet
- Vaccine Guide - Randall NeustaedterDocument6 pagesVaccine Guide - Randall NeustaedterttreksNo ratings yet
- (GYNE) Ovarian Neoplasms-Dr. Delos Reyes (MRA)Document9 pages(GYNE) Ovarian Neoplasms-Dr. Delos Reyes (MRA)adrian kristopher dela cruzNo ratings yet
- Introduction To Preventive and Community MedicineDocument2 pagesIntroduction To Preventive and Community MedicineMonsour SalazarNo ratings yet
- Nursing Management of HypertensionDocument152 pagesNursing Management of HypertensionEnfermeriaAncam100% (3)
- Consti and Juris Cases Compilation 3Document169 pagesConsti and Juris Cases Compilation 3MG DangtayanNo ratings yet
- Bacterial Transformation Lab ReportDocument11 pagesBacterial Transformation Lab ReportRichie JustinNo ratings yet
- Library Catalogue MIMU Apr2016Document599 pagesLibrary Catalogue MIMU Apr2016Ye Tun AungNo ratings yet
- Lennon Et Al. 2018 - Framework To Construct and Interpret Latent Class Trajectory ModellingDocument10 pagesLennon Et Al. 2018 - Framework To Construct and Interpret Latent Class Trajectory ModellingPsic. Dra. Marina MorenoNo ratings yet
- Care PlanDocument3 pagesCare PlanMarlene Mathew100% (1)
- Respiratory Distress Syndrome Hmd-Ttnb-Mas-Neonatal PneumoniaDocument65 pagesRespiratory Distress Syndrome Hmd-Ttnb-Mas-Neonatal PneumoniaBLOBLOBNo ratings yet
- RUQYAH AND MEDICINE by Sheilkabdul RaoufDocument3 pagesRUQYAH AND MEDICINE by Sheilkabdul RaoufAhmed MagajiNo ratings yet
- SCIENCE 10 Genetics Worksheets With Answers 1Document4 pagesSCIENCE 10 Genetics Worksheets With Answers 1Anngela Arevalo Barcenas100% (1)
- Difference Between Case Study and Literature ReviewDocument6 pagesDifference Between Case Study and Literature Reviewea5zjs6aNo ratings yet
- General Anaesthesia MCQsDocument5 pagesGeneral Anaesthesia MCQsWasi Khan100% (3)
- Go Go Go First Vita PlusDocument6 pagesGo Go Go First Vita PlusArnulfo Yu LanibaNo ratings yet
- Maternity Exam 2Document56 pagesMaternity Exam 2Johanna Erazo Padilla80% (10)
- Laporan Pemakaian Dan Lembar Permintaan Reagen (LPLPR)Document8 pagesLaporan Pemakaian Dan Lembar Permintaan Reagen (LPLPR)Juli Anggarawati ChanelNo ratings yet
- Ogd Colonoscopy Day Surgery or Hospital Admission Consultation FormDocument3 pagesOgd Colonoscopy Day Surgery or Hospital Admission Consultation FormMartin StephanNo ratings yet
- Hot Dog Cart Manual SAMPLEDocument6 pagesHot Dog Cart Manual SAMPLETrina Nuguid100% (1)
- 2 Oral UlcersDocument27 pages2 Oral UlcersAhmed Abdelhady Mahmoud AbdelwahedNo ratings yet
- History of MedicineDocument24 pagesHistory of MedicineРоман КравецьNo ratings yet
- Vii. Nursing Care Plan: Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument2 pagesVii. Nursing Care Plan: Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveMezil NazarenoNo ratings yet