You might also like
- Periprosthetic Infection: Farry, DRDocument15 pagesPeriprosthetic Infection: Farry, DRFarry DoankNo ratings yet
- SSI PrventionDocument27 pagesSSI PrventionIPC PFKCCNo ratings yet
- TB Meningitis Lancet 2022Document15 pagesTB Meningitis Lancet 2022stephanie bojorquezNo ratings yet
- 2midterm 8 - Diagnostic Virology TRANSDocument2 pages2midterm 8 - Diagnostic Virology TRANSRobee Camille Desabelle-SumatraNo ratings yet
- Discuss The Pathogenesis and Management of Periprosthetic Joint InfectionDocument30 pagesDiscuss The Pathogenesis and Management of Periprosthetic Joint InfectionNURA MUHAMMAD ALIYUNo ratings yet
- 2-Microscopic IdentificationDocument24 pages2-Microscopic IdentificationMunir AhmedNo ratings yet
- Adenoviruses - Medical Microbiology - NCBI Bookshelf PDFDocument9 pagesAdenoviruses - Medical Microbiology - NCBI Bookshelf PDFNino MwansahNo ratings yet
- Virology Techniques: Chapter 5 - Lesson 4Document8 pagesVirology Techniques: Chapter 5 - Lesson 4Ramling PatrakarNo ratings yet
- Bacteria: Acid Fast Bacilli: Nama Karakteristi K Manifestasi Klinis Struktur Antigen + Enzim + Toxin Diagnosis TerapiDocument2 pagesBacteria: Acid Fast Bacilli: Nama Karakteristi K Manifestasi Klinis Struktur Antigen + Enzim + Toxin Diagnosis TerapiAndreas MoekoeNo ratings yet
- Tes Lab Penyakit Infeksi Dan Tropis (April 2011)Document143 pagesTes Lab Penyakit Infeksi Dan Tropis (April 2011)Fajrul AnsarNo ratings yet
- Kumpulan Jurnal DengueDocument122 pagesKumpulan Jurnal DengueMas MantriNo ratings yet
- Bacterial Meningitis and Brain Abscess: Key PointsDocument7 pagesBacterial Meningitis and Brain Abscess: Key PointsMartha OktaviaNo ratings yet
- I Viral DiseasesDocument41 pagesI Viral DiseasesSagar AcharyaNo ratings yet
- Microbiology '' Microbiology-Clinical Bacteriology Microbiology '' Microbiology-Clinical Bacteriology Section IiDocument8 pagesMicrobiology '' Microbiology-Clinical Bacteriology Microbiology '' Microbiology-Clinical Bacteriology Section IiHanunNo ratings yet
- Gram negative pathogens and the diseases they causeDocument72 pagesGram negative pathogens and the diseases they causelathaNo ratings yet
- Surgical Site Infection DR WidDocument36 pagesSurgical Site Infection DR WidNia UswantiNo ratings yet
- Diabetic Foot JAAOSDocument8 pagesDiabetic Foot JAAOSAtikah ZuraNo ratings yet
- Microbiology: Case 1 Bacterial Wound InfectionsDocument11 pagesMicrobiology: Case 1 Bacterial Wound InfectionsNIMMAGADDA, KETHANANo ratings yet
- Surgical Site Infection GuideDocument41 pagesSurgical Site Infection GuideJawad Mustafa100% (1)
- Musculoskeletal InfectionsDocument12 pagesMusculoskeletal InfectionsSetiawan Suseno100% (1)
- Actinomyces & Nocardia 06-07-MedDocument11 pagesActinomyces & Nocardia 06-07-Medapi-3699361No ratings yet
- DiphteriaDocument64 pagesDiphteriaOmarNo ratings yet
- Actinomycosis: Mohanad N. Saleh 6 Year Meical Student Supervisor: Dr. Anas MuhannaDocument19 pagesActinomycosis: Mohanad N. Saleh 6 Year Meical Student Supervisor: Dr. Anas MuhannaMohanad SalehNo ratings yet
- Lecture 27-Basic Virology-Dr. Ludhang Pradipta Rizki, M.biotech, SP - MK (2018)Document45 pagesLecture 27-Basic Virology-Dr. Ludhang Pradipta Rizki, M.biotech, SP - MK (2018)NOVI UMAMI UMAMINo ratings yet
- Surgical Wound Infection GuideDocument6 pagesSurgical Wound Infection GuideTeddy MuaNo ratings yet
- Fever With Rash SeminarDocument98 pagesFever With Rash SeminarSYAZRIANA SUHAIMINo ratings yet
- Introduction of MGIT Liquid & InstrumentDocument56 pagesIntroduction of MGIT Liquid & InstrumentRosantia SarassariNo ratings yet
- Herpes Zoster (Shingles) : Muhammad Abdullah Dept. of Dermatology DHQ Hospital FaisalabadDocument26 pagesHerpes Zoster (Shingles) : Muhammad Abdullah Dept. of Dermatology DHQ Hospital FaisalabadwaleedNo ratings yet
- Brucellosis: A Highly Contagious Zoonotic DiseaseDocument55 pagesBrucellosis: A Highly Contagious Zoonotic Diseasesana shakeelNo ratings yet
- Guidelines of Surgical Site InfectionsDocument33 pagesGuidelines of Surgical Site InfectionsAndrie KundrieNo ratings yet
- Pedoman Necrotizing EnterocolitisDocument10 pagesPedoman Necrotizing EnterocolitisMuhamad Zulfatul A'laNo ratings yet
- HO - Dengue VirusDocument2 pagesHO - Dengue VirusSigop Elliot LNo ratings yet
- Influenza: DR.T .V.R Ao MDDocument81 pagesInfluenza: DR.T .V.R Ao MDtummalapalli venkateswara raoNo ratings yet
- Genexpert Ultra JC FinalDocument41 pagesGenexpert Ultra JC FinalmeghaNo ratings yet
- SpirocheteDocument32 pagesSpirocheteSAYMABANUNo ratings yet
- Malaria: Immunology and ImmunizationFrom EverandMalaria: Immunology and ImmunizationJulius P. KreierNo ratings yet
- Spirochetes: Aashutosh Nama M.SC Microbiology Sem - 1 Dr. B Lal Institute of BiotechnologyDocument34 pagesSpirochetes: Aashutosh Nama M.SC Microbiology Sem - 1 Dr. B Lal Institute of Biotechnologyaashutosh namaNo ratings yet
- Immunity To MicrobesDocument25 pagesImmunity To MicrobestimcarasNo ratings yet
- Tuberculosis en PDFDocument307 pagesTuberculosis en PDFAbdullah Khairul AfnanNo ratings yet
- MycetomaDocument26 pagesMycetomaTummalapalli Venkateswara RaoNo ratings yet
- Scrub TyphusDocument2 pagesScrub TyphusitsankurzNo ratings yet
- Intestinal Coccidian ParasitesDocument23 pagesIntestinal Coccidian ParasitesABC100% (1)
- Meningitis In Children: Signs, Symptoms And TreatmentDocument48 pagesMeningitis In Children: Signs, Symptoms And TreatmentAli FalihNo ratings yet
- Myco - 05 - Dermatophyte & AsperagillusDocument92 pagesMyco - 05 - Dermatophyte & AsperagillusesraaNo ratings yet
- Septic Arthritis & OsteomyelitisDocument42 pagesSeptic Arthritis & OsteomyelitisCabdi WaliNo ratings yet
- Tuberculosis BasicsDocument95 pagesTuberculosis Basicstummalapalli venkateswara rao100% (1)
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocument18 pagesMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaNo ratings yet
- 1 Staphylococcus Lecture 1 Last YearDocument39 pages1 Staphylococcus Lecture 1 Last YearKeshant Samaroo100% (1)
- Infectious Disease Study Guide 2Document32 pagesInfectious Disease Study Guide 2Jim GoetzNo ratings yet
- CMV VirusDocument8 pagesCMV VirusKalpavriksha1974No ratings yet
- Gilut Herpes ZosteRDocument24 pagesGilut Herpes ZosteRdimasahadiantoNo ratings yet
- Infectious Diseases - Infective EndocarditisDocument41 pagesInfectious Diseases - Infective Endocarditisfire_n_iceNo ratings yet
- Malaria 25 03 09Document131 pagesMalaria 25 03 09Dr.Jagadish Nuchina100% (5)
- Pseudomonas BasicsDocument32 pagesPseudomonas Basicstummalapalli venkateswara raoNo ratings yet
- Discuss The Role of Immunology in SurgeryDocument16 pagesDiscuss The Role of Immunology in SurgeryrosybashNo ratings yet
- Hiv PPDocument37 pagesHiv PPJitendra YadavNo ratings yet
- Tetanu S: By: Reno WaisyahDocument18 pagesTetanu S: By: Reno WaisyahReno WaisyahNo ratings yet
- Histology Saraf2Document1 pageHistology Saraf2reno waisyahNo ratings yet
- Histology Saraf1 PDFDocument1 pageHistology Saraf1 PDFreno waisyahNo ratings yet
- Melamine Contaminated Powdered Formula and Urolithiasis in Young ChildrenDocument8 pagesMelamine Contaminated Powdered Formula and Urolithiasis in Young ChildrenReno WaisyahNo ratings yet
- Bacterial Diarrhea: Clinical PracticeDocument10 pagesBacterial Diarrhea: Clinical PracticeReno WaisyahNo ratings yet
- Telenursing: The Future of Transforming CareDocument10 pagesTelenursing: The Future of Transforming CareSujatha J JayabalNo ratings yet
- History Patient - Co.ukDocument14 pagesHistory Patient - Co.ukiuytrerNo ratings yet
- 17 TYPES OF GOOD BACTERIA - The List of Most Beneficial Species of Probiotics Lactobacillus and Bifidobacteria - Ecosh LifeDocument30 pages17 TYPES OF GOOD BACTERIA - The List of Most Beneficial Species of Probiotics Lactobacillus and Bifidobacteria - Ecosh LifeCarl MacCordNo ratings yet
- Fixed Prosthodontics: Drg. Bertha E. Setio, SpprosDocument16 pagesFixed Prosthodontics: Drg. Bertha E. Setio, Spprosiin revient29No ratings yet
- Research Paper-Hlth1050Document5 pagesResearch Paper-Hlth1050api-691549090No ratings yet
- Emergency Medicine ST3 DRE-EM - 2024 Alternative CertificateDocument8 pagesEmergency Medicine ST3 DRE-EM - 2024 Alternative Certificateiffi82No ratings yet
- Improve Nursing Skills and Knowledge with Medical Case Studies and QuestionsDocument41 pagesImprove Nursing Skills and Knowledge with Medical Case Studies and Questionsjodymahmoud100% (1)
- Asante Teaching Hospital Activity Based CostingDocument3 pagesAsante Teaching Hospital Activity Based CostingMuskanNo ratings yet
- cs3 Protocol-V2.5Document8 pagescs3 Protocol-V2.5CheferishNo ratings yet
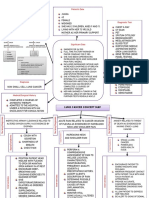
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- NCM 107 Postpartum Care Guide QuestionDocument6 pagesNCM 107 Postpartum Care Guide QuestionMiguel LigasNo ratings yet
- Pamphlet TemplateDocument2 pagesPamphlet TemplateZoe ColemanNo ratings yet
- RasproDocument63 pagesRasprofany hertinNo ratings yet
- CRC Model Group-7Document11 pagesCRC Model Group-7Misganaw TadesseNo ratings yet
- PT job descriptionDocument3 pagesPT job descriptionFaer PangilinanNo ratings yet
- Acute & Chronic Rhinitis Types, Symptoms, TreatmentsDocument19 pagesAcute & Chronic Rhinitis Types, Symptoms, TreatmentsAdilah RadziNo ratings yet
- Acute MastitisDocument2 pagesAcute MastitisFatima TsannyNo ratings yet
- Sorbion SachetsDocument3 pagesSorbion SachetsReil_InsulaNo ratings yet
- Rasha Hamdy CVDocument6 pagesRasha Hamdy CVH1552000No ratings yet
- Fluids and Electrolytes in ElderlyDocument7 pagesFluids and Electrolytes in ElderlyDithaNo ratings yet
- Daleel EDocument44 pagesDaleel Ealiplus007No ratings yet
- Ilovepdf MergedDocument53 pagesIlovepdf MergedJoel CalapiñaNo ratings yet
- Type of Hospital AdmissionDocument2 pagesType of Hospital AdmissionPenugasan PerpanjanganNo ratings yet
- Optima Health 2023 2024 Cova - Benefits Brochure FinalDocument8 pagesOptima Health 2023 2024 Cova - Benefits Brochure FinalKobusNo ratings yet
- PelajaranDocument25 pagesPelajaranmarisa isahNo ratings yet
- Test Bank Chapter 5: Patient and Family Teaching: Lewis: Medical-Surgical Nursing, 7 EditionDocument8 pagesTest Bank Chapter 5: Patient and Family Teaching: Lewis: Medical-Surgical Nursing, 7 EditionBriseidaSolisNo ratings yet
- Journal Maria F Delong - Impact of Plaque Burden Vs Stenosis On Ischemic Events in Patient With Coronary AtherosclerosisDocument20 pagesJournal Maria F Delong - Impact of Plaque Burden Vs Stenosis On Ischemic Events in Patient With Coronary AtherosclerosisAris MarutoNo ratings yet
- A Family Physician's Perspective On Vaccine Hesitancy: Margot Savoy, MD, MPH, FaafpDocument6 pagesA Family Physician's Perspective On Vaccine Hesitancy: Margot Savoy, MD, MPH, FaafpNational Press FoundationNo ratings yet
- Literature Review On Hepatitis B and CDocument10 pagesLiterature Review On Hepatitis B and Cafmzyywqyfolhp100% (1)
- Clinical Approach in Generalized Pustular Psoriasis One Case Report 63a04e949936aDocument8 pagesClinical Approach in Generalized Pustular Psoriasis One Case Report 63a04e949936aThomas UtomoNo ratings yet