You might also like
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- What Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inDocument6 pagesWhat Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inAnnapoorna SHNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathyAnonymous GIGXKjfLNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Acute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusDocument3 pagesAcute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusKristine Danielle DejeloNo ratings yet
- Case Study For Chronic Renal FailureDocument6 pagesCase Study For Chronic Renal FailureGabbii CincoNo ratings yet
- Glomerulonephritis: Marivic J. MiagarDocument28 pagesGlomerulonephritis: Marivic J. MiagarMarivic DianoNo ratings yet
- CASE STUDY FORMAT (Kidney Transplantation)Document12 pagesCASE STUDY FORMAT (Kidney Transplantation)ashnaNo ratings yet
- Respiratory Distress in NewbornDocument52 pagesRespiratory Distress in NewbornNadia SalwaniNo ratings yet
- City of Manila (Formerly City College of Manila) Mehan Gardens, ManilaDocument8 pagesCity of Manila (Formerly City College of Manila) Mehan Gardens, Manilaicecreamcone_201No ratings yet
- Electrolyte Imbalance in ElderlyDocument70 pagesElectrolyte Imbalance in ElderlyPrasannakumar P CNo ratings yet
- NCP Poststreptococcal GlomerulonephritisDocument12 pagesNCP Poststreptococcal GlomerulonephritisScarlet ScarletNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Peritoneal DialysisDocument3 pagesPeritoneal DialysisSumit YadavNo ratings yet
- Pathophysiology of Malaria: How Parasite Infection Affects the BodyDocument20 pagesPathophysiology of Malaria: How Parasite Infection Affects the Bodymelia100% (1)
- Edema: Dr. Bernardo Dámaso MataDocument55 pagesEdema: Dr. Bernardo Dámaso MataDeivis Dan ErickNo ratings yet
- Pathological Changes of DM - 2023Document53 pagesPathological Changes of DM - 2023Visura PrabodNo ratings yet
- Nephrotic SyndromeeDocument28 pagesNephrotic SyndromeeRiteka SinghNo ratings yet
- Patterns of Nursing Care Delivery in IndiaDocument22 pagesPatterns of Nursing Care Delivery in IndiaBinu JoshvaNo ratings yet
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399No ratings yet
- Glomerulonephritis vs GlomerulopathiesDocument58 pagesGlomerulonephritis vs GlomerulopathiesRahmailla Khanza Diana FebriliantriNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument8 pagesIdiopathic Thrombocytopenic PurpuraMonette Abalos MendovaNo ratings yet
- Aklan State University Nursing Readings on Pyloric StenosisDocument5 pagesAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
- MR Elamin ShockDocument70 pagesMR Elamin ShockMohammed Abd AlgadirNo ratings yet
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 pagesPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNo ratings yet
- Nephrotic and Nephritic SyndromesDocument27 pagesNephrotic and Nephritic SyndromesJoshua Smith100% (1)
- Congenital Heart DiseaseDocument12 pagesCongenital Heart Diseaserakanootousan100% (1)
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Acute GlomerulonephritisDocument17 pagesAcute GlomerulonephritisBayanSecond WardNo ratings yet
- Understanding Epilepsy: Causes, Types, and TreatmentDocument10 pagesUnderstanding Epilepsy: Causes, Types, and TreatmentRegineCuasSulibNo ratings yet
- CKD Overview: Causes, Symptoms and Stages of Chronic Kidney DiseaseDocument15 pagesCKD Overview: Causes, Symptoms and Stages of Chronic Kidney Diseasejames100% (1)
- Glomerulonephritis 10Document5 pagesGlomerulonephritis 10Eden Jay Calija AgoyNo ratings yet
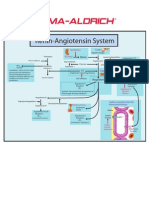
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Pericardial EffusionDocument36 pagesPericardial EffusionRizky Amalia Wakano100% (1)
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapyShelly Dwi SilvitaNo ratings yet
- Medscape Status EpilepticusDocument10 pagesMedscape Status EpilepticusEllen Siska SusantiNo ratings yet
- PericarditisDocument11 pagesPericarditisrbarcellonaNo ratings yet
- HemodialysisDocument11 pagesHemodialysisjuan_sioNo ratings yet
- Pathophysiology of ArrhythmiasDocument15 pagesPathophysiology of ArrhythmiasJonathan MontecilloNo ratings yet
- Chronic Kidney DiseaseDocument7 pagesChronic Kidney DiseaseLardel Balbiran LafortezaNo ratings yet
- Hypertension: Mayur BV BPH 3 Semester PSPHDocument29 pagesHypertension: Mayur BV BPH 3 Semester PSPHBijay Kumar MahatoNo ratings yet
- GlomerulonephritisDocument8 pagesGlomerulonephritisMatthew Ryan100% (1)
- Tropical Splenomegaly SyndromeDocument12 pagesTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Anaphylactic ReactionDocument9 pagesAnaphylactic ReactionZahir Jayvee Gayak IINo ratings yet
- Congenital SyphilisDocument6 pagesCongenital SyphilisFrozen Pandora MahayaNo ratings yet
- Disseminated Intravascular CoagulationDocument2 pagesDisseminated Intravascular CoagulationVince100% (1)
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesNo ratings yet
- Purpura and Petechiae: Symptoms and Types of Idiopathic Thrombocytopenic Purpura (ITPDocument7 pagesPurpura and Petechiae: Symptoms and Types of Idiopathic Thrombocytopenic Purpura (ITPMarie Joe AbainzaNo ratings yet
- Pyloric Stenosis GuideDocument5 pagesPyloric Stenosis GuideMichael AlexanderNo ratings yet
- Anemia of Chronic Disease - Inflammation - UpToDateDocument36 pagesAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloNo ratings yet
- Poststreptococcal Glomerulonephritis - UpToDateDocument21 pagesPoststreptococcal Glomerulonephritis - UpToDateHandre Putra100% (1)
- Case Studies - Tetralogy of FallotDocument16 pagesCase Studies - Tetralogy of FallotKunwar Sidharth SaurabhNo ratings yet
- Paediatric Diabetic KetoacidosisDocument7 pagesPaediatric Diabetic KetoacidosisJuan Carlos BayonaNo ratings yet
- Pathophysiology of ESRD: Organ Dysfunctions & Associated AbnormalitiesDocument5 pagesPathophysiology of ESRD: Organ Dysfunctions & Associated AbnormalitiesCarl JardelezaNo ratings yet
- Exudative Pleural Effusions - UpToDateDocument2 pagesExudative Pleural Effusions - UpToDateAsif IqbalNo ratings yet
- Nepro GNDocument6 pagesNepro GNHajime NakaegawaNo ratings yet
- Lecture 10 AutoimmunityDocument78 pagesLecture 10 AutoimmunitytimcarasNo ratings yet
- Visual Guide to Understanding Lupus Symptoms and TreatmentsDocument17 pagesVisual Guide to Understanding Lupus Symptoms and Treatmentsgilbie1402No ratings yet
- 2016 Imitadores de PreeclmapsiaDocument9 pages2016 Imitadores de PreeclmapsiaMaria del Pilar Devis MoralesNo ratings yet
- Autoimmune DiseasesDocument14 pagesAutoimmune Diseasesdr_swaralipiNo ratings yet
- The EULAR Report 2017 LoresDocument50 pagesThe EULAR Report 2017 Loresrca ieftinNo ratings yet
- Presented By: Dr. Hirdesh Chawla Junior Resident IiiDocument79 pagesPresented By: Dr. Hirdesh Chawla Junior Resident IiiAzizan HannyNo ratings yet
- An Update On Glomerulopathies - Clinical and Treatment AspectsDocument482 pagesAn Update On Glomerulopathies - Clinical and Treatment AspectsJulio SobremazasNo ratings yet
- Psicopatología Del LupusDocument6 pagesPsicopatología Del LupusEsteban VediaNo ratings yet
- cSLE 2018 GuidelinesDocument6 pagescSLE 2018 GuidelinesJPNo ratings yet
- VN Shegal Textbook of Clinical Dermatology 5th Edition PDFDocument365 pagesVN Shegal Textbook of Clinical Dermatology 5th Edition PDFdianaurs1823100% (2)
- Immuno TB Flashcards Unit 3Document7 pagesImmuno TB Flashcards Unit 3shahzebNo ratings yet
- Environmental Factors and Clinical Manifestations of Systemic Lupus ErythematosusDocument1 pageEnvironmental Factors and Clinical Manifestations of Systemic Lupus ErythematosusMel Izhra N. MargateNo ratings yet
- Systemic Lupus Erythematosus - Immunity PDFDocument7 pagesSystemic Lupus Erythematosus - Immunity PDFTõkå MøhámmêdNo ratings yet
- Dr Saif Darif's Guide to Rheumatic DiseasesDocument30 pagesDr Saif Darif's Guide to Rheumatic DiseasesMohamed A SalehNo ratings yet
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuNo ratings yet
- Physical Sigs in General Medicine 2edDocument211 pagesPhysical Sigs in General Medicine 2edStacy Smith100% (24)
- Antiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositaDocument9 pagesAntiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositadidongNo ratings yet
- 0009 Rheumatology Notes 2015 PDFDocument56 pages0009 Rheumatology Notes 2015 PDFMuhammad HaneefNo ratings yet
- Common Medical Abbreviations: SUB Script SubscriptDocument10 pagesCommon Medical Abbreviations: SUB Script SubscriptYing Jie LiowNo ratings yet
- MCQs 1Document10 pagesMCQs 1Mostafa MahmoudNo ratings yet
- Magnesium Sulfate Drug StudyDocument2 pagesMagnesium Sulfate Drug StudyMaan Molinyawe81% (16)
- DR Ebrahim CK Notes PDFDocument149 pagesDR Ebrahim CK Notes PDFWendy MaeNo ratings yet
- Approach To Patients EULARDocument35 pagesApproach To Patients EULARstuckinbedNo ratings yet
- ArchRheumatol 32 21Document5 pagesArchRheumatol 32 21indriNo ratings yet
- Systemic Lupus Erythematosus Quality of Life Questionnaire: Identifier NoDocument3 pagesSystemic Lupus Erythematosus Quality of Life Questionnaire: Identifier NoDwi MahendraNo ratings yet
- 50 Shades of Practice QuestionsDocument11 pages50 Shades of Practice QuestionsAmie Ray100% (1)
- A Lecture Schedule, July 2015-June 2016Document12 pagesA Lecture Schedule, July 2015-June 2016Shahriar Kabir DaneNo ratings yet
- Musculoskeletal Exam Questions PortfolioDocument7 pagesMusculoskeletal Exam Questions Portfolioapi-360345296No ratings yet
- Peds HemeImmune OUTLINEDocument10 pagesPeds HemeImmune OUTLINEAshleyNo ratings yet
- Understanding Arthritis: Key Factors in Differential DiagnosisDocument10 pagesUnderstanding Arthritis: Key Factors in Differential DiagnosisshosmedNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)