You might also like
- Hypothyroidism: Kommerien Daling, MD Chiefs Conference August 14th 2008Document50 pagesHypothyroidism: Kommerien Daling, MD Chiefs Conference August 14th 2008HaNy NejNo ratings yet
- Congenital HypothyroidismDocument21 pagesCongenital HypothyroidismDanna GarcíaNo ratings yet
- Dermatological and Haemato-Biochemical Characteristics of Canine HypothyroidismDocument5 pagesDermatological and Haemato-Biochemical Characteristics of Canine HypothyroidismsumNo ratings yet
- HES2125 10S2 Revision01Document4 pagesHES2125 10S2 Revision01Roberto RizzoNo ratings yet
- Hashimoto ThyroiditisDocument6 pagesHashimoto Thyroiditismananginsiang100% (1)
- Sumerian AchievementsDocument5 pagesSumerian AchievementsmagilNo ratings yet
- Thyroid Disease AlgorithmsDocument29 pagesThyroid Disease AlgorithmsGoh Chong Aik100% (2)
- Obg Lesson Plan ObgDocument8 pagesObg Lesson Plan ObgPriyanka SheoranNo ratings yet
- Nqs PLP E-Newsletter No45Document4 pagesNqs PLP E-Newsletter No45api-302273256No ratings yet
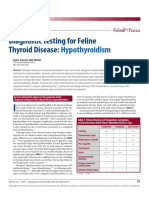
- Testing For HypothyroidismDocument23 pagesTesting For HypothyroidismFlávia UchôaNo ratings yet
- Equine Thyroid DysfunctionDocument15 pagesEquine Thyroid DysfunctionDirección Científica Laboratorio VitalabNo ratings yet
- Peterson 2007Document13 pagesPeterson 2007Luisa Fernanda Rojas DiazNo ratings yet
- Inc Prevalnce Retrospective Evidence 1994 PetersonDocument25 pagesInc Prevalnce Retrospective Evidence 1994 PetersonKurt SciclunaNo ratings yet
- Kurniawan 2020Document6 pagesKurniawan 2020PPDS ANAK FK USUNo ratings yet
- Graves Disease - StatPearls - NCBI BookshelfDocument8 pagesGraves Disease - StatPearls - NCBI BookshelfDr.Pradip PatilNo ratings yet
- Graves' Disease: Graves' Disease Is An Autoimmune Disease Where The Thyroid IsDocument6 pagesGraves' Disease: Graves' Disease Is An Autoimmune Disease Where The Thyroid IsMoof06No ratings yet
- Pathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis)Document31 pagesPathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis)Juan Sebastian Carrillo GomezNo ratings yet
- Goitre Et Nodule ThyrogdienDocument4 pagesGoitre Et Nodule ThyrogdienKeishaNo ratings yet
- Central Hypothyroidism: Pathogenic, Diagnostic, and Therapeutic ChallengesDocument11 pagesCentral Hypothyroidism: Pathogenic, Diagnostic, and Therapeutic ChallengesCroitort53No ratings yet
- Thyroid-Associated Ophthalmopathy: ReviewDocument12 pagesThyroid-Associated Ophthalmopathy: Reviewkevin_jawanNo ratings yet
- Apa Apa AjaDocument15 pagesApa Apa AjaAdelaida PurwantaNo ratings yet
- Annals of Medicine and SurgeryDocument3 pagesAnnals of Medicine and SurgeryUsee TvNo ratings yet
- Thyroid Disorders in The Geriatric Patient: Susan A. Meeking, DVMDocument19 pagesThyroid Disorders in The Geriatric Patient: Susan A. Meeking, DVMMaria Alice BourneufNo ratings yet
- Lesson 2: Chemical Pathology of The ThyroidDocument2 pagesLesson 2: Chemical Pathology of The ThyroidAntony WaithakaNo ratings yet
- EJHM - Volume 71 - Issue 1 - Pages 2250-2252Document3 pagesEJHM - Volume 71 - Issue 1 - Pages 2250-2252Nermin AbdelnabyNo ratings yet
- Canine Hypothyreoidism: Clinical SignsDocument4 pagesCanine Hypothyreoidism: Clinical Signsreerwrr qeqweNo ratings yet
- The Pathogenesis of Hashimoto's Thyroiditis: Further Developments in Our UnderstandingDocument9 pagesThe Pathogenesis of Hashimoto's Thyroiditis: Further Developments in Our UnderstandingXochil RmzNo ratings yet
- Goiter: Signs and Symptoms of GoitersDocument15 pagesGoiter: Signs and Symptoms of GoitersGraceLanaNo ratings yet
- Title: Congenital Hypothyroidism: A Ran Sacker Escaping Under The Nose AbstractDocument6 pagesTitle: Congenital Hypothyroidism: A Ran Sacker Escaping Under The Nose AbstractKavita KhannaNo ratings yet
- Canine Hypothyroidism, An OverviewDocument6 pagesCanine Hypothyroidism, An OverviewISABELSSBNo ratings yet
- D'Aurizio Et Al - Free Thyroxine Measurement in Clinical Practice How To Optimize Indications Analytical Procedures and Interpretation Criteria While Waiting ForDocument41 pagesD'Aurizio Et Al - Free Thyroxine Measurement in Clinical Practice How To Optimize Indications Analytical Procedures and Interpretation Criteria While Waiting ForerixNo ratings yet
- A. Brief Definition of The Specific Disease Condition: Mechanism CauseDocument6 pagesA. Brief Definition of The Specific Disease Condition: Mechanism CauseEuniceNo ratings yet
- Distinct Histopathological Features of Hashimoto'S Thyroiditis With Respect To Igg4-Related DiseaseDocument12 pagesDistinct Histopathological Features of Hashimoto'S Thyroiditis With Respect To Igg4-Related DiseaseRifqi Fathul ArroisiNo ratings yet
- Hypo Thyroid Is MDocument75 pagesHypo Thyroid Is Mbiniam MesfinNo ratings yet
- Clinicopathological Study of Hashimoto Thyroiditis: Pooja Jain, Geetha Vasudevan, Kanthilata PaiDocument5 pagesClinicopathological Study of Hashimoto Thyroiditis: Pooja Jain, Geetha Vasudevan, Kanthilata PaiRifqi Fathul ArroisiNo ratings yet
- PSM 1 Peterson PDFDocument6 pagesPSM 1 Peterson PDFMaria Rodriguez RodrguezNo ratings yet
- Hypothyroid ScreeningDocument8 pagesHypothyroid ScreeningPradeep DeivasigamaniNo ratings yet
- Hypothyroidism - StatPearls - NCBI BookshelfDocument10 pagesHypothyroidism - StatPearls - NCBI BookshelfKarla CordobaNo ratings yet
- Canine Thyroid and Autoimmune DiseaseDocument20 pagesCanine Thyroid and Autoimmune DiseasepimpimismeNo ratings yet
- Rawalpindi Army Hosp HypothyDocument5 pagesRawalpindi Army Hosp Hypothyhinduja reddipilliNo ratings yet
- Laboratory Assesment of Thyroid Function PMC2003Document14 pagesLaboratory Assesment of Thyroid Function PMC2003Muhammad Dadan KurniawanNo ratings yet
- Dodds On Thyroid4Document12 pagesDodds On Thyroid4Saad MotawéaNo ratings yet
- Primary HyperparathyroidismDocument9 pagesPrimary HyperparathyroidismJamesNo ratings yet
- Pathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDateDocument22 pagesPathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDaterazvanNo ratings yet
- Hypoadrenocorticism in A Young Dwarf Cat - Case ReportDocument10 pagesHypoadrenocorticism in A Young Dwarf Cat - Case ReportHerry Wildan FawziNo ratings yet
- NTU BS3104 Endocrine NotesDocument116 pagesNTU BS3104 Endocrine NotesChen HouyuNo ratings yet
- Bulowpedersen 2005Document8 pagesBulowpedersen 2005MariaLyNguyễnNo ratings yet
- Congenital HypothyroidismDocument36 pagesCongenital HypothyroidismRandi DwiyantoNo ratings yet
- Hypo Thyroid Is MDocument15 pagesHypo Thyroid Is MbonogulNo ratings yet
- American Thyroid Association Guidelines For Detection of Thyroid DysfunctionDocument5 pagesAmerican Thyroid Association Guidelines For Detection of Thyroid DysfunctionUdsanee SukpimonphanNo ratings yet
- Chapter 128 - Thyroid and Adrenal Disorders: Episode OverviewDocument15 pagesChapter 128 - Thyroid and Adrenal Disorders: Episode OverviewIkenna EzeiloNo ratings yet
- Subclinicsl HyperthyroidismDocument9 pagesSubclinicsl HyperthyroidismDudella Desnani Firman YasinNo ratings yet
- 1 s2.0 S1726490114002603 MainDocument9 pages1 s2.0 S1726490114002603 Mainmagelang utaraNo ratings yet
- Thyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. AvinashDocument9 pagesThyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. Avinashbelakang rumahNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument12 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- 1 2 3 4 MergedDocument20 pages1 2 3 4 Mergedcataleya mesaNo ratings yet
- Wassner 2018Document18 pagesWassner 2018brendavanessameraaNo ratings yet
- PokhrelDocument9 pagesPokhrelsaifulmangopo123No ratings yet
- The Diagnosis and Management of Central Hypothyroidism in 2018Document11 pagesThe Diagnosis and Management of Central Hypothyroidism in 2018fighter dreamNo ratings yet
- Hypothyroidism: Special Types of HypothyroidismDocument4 pagesHypothyroidism: Special Types of HypothyroidismVictor VicencioNo ratings yet
- Power Policy of MeghalayaDocument39 pagesPower Policy of MeghalayacbbindiaNo ratings yet
- Ao 2016 046 Final ReportDocument15 pagesAo 2016 046 Final ReportrenoguNo ratings yet
- Soal Pas B. Ingg Ix 2223 GanjilDocument7 pagesSoal Pas B. Ingg Ix 2223 GanjilvitriNo ratings yet
- BSBPMG521 Assessment Task 2Document13 pagesBSBPMG521 Assessment Task 2Blessie PialaNo ratings yet
- The Values of An AugustinianDocument1 pageThe Values of An AugustinianCarla VirtucioNo ratings yet
- Characterization of Models For Time-Dependent Behavior of SoilsDocument21 pagesCharacterization of Models For Time-Dependent Behavior of SoilsrkNo ratings yet
- Accommodation Costs 2023-2024 With Lease DatesDocument1 pageAccommodation Costs 2023-2024 With Lease DatesMadalongipolahaNo ratings yet
- Aqua-K-Othrine Insecticide Space-Spray Concentrate SDS GHS 1016Document11 pagesAqua-K-Othrine Insecticide Space-Spray Concentrate SDS GHS 1016Juan Carlos ParamoNo ratings yet
- Prospect SRSKerlaDocument23 pagesProspect SRSKerlaSonal ShahNo ratings yet
- Original Complaint Doc1 Redwood Dental Group vs. American Dental PartnersDocument144 pagesOriginal Complaint Doc1 Redwood Dental Group vs. American Dental PartnersDGardner242No ratings yet
- HRIS Implementation in Organizations IssDocument7 pagesHRIS Implementation in Organizations IssMary Grace BuotNo ratings yet
- Betty Neuman: The System ModelDocument32 pagesBetty Neuman: The System ModelVincent PolicarNo ratings yet
- Exams Briefing For Final Year Students Spring 2021Document30 pagesExams Briefing For Final Year Students Spring 2021Van TeaNo ratings yet
- Ciclostomi FosiliDocument5 pagesCiclostomi FosiliAnca MihalcescuNo ratings yet
- HDL WorkerDocument22 pagesHDL Workershravan oracleNo ratings yet
- Placement Write UpsDocument2 pagesPlacement Write UpsSourish NagNo ratings yet
- Daily Lesson PlanDocument1 pageDaily Lesson Planjason.bedell100% (1)
- Political ScienceDocument23 pagesPolitical ScienceR.Sowmya ReddyNo ratings yet
- September 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityDocument23 pagesSeptember 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityEzekiel GantiedNo ratings yet
- From Ef Cient Markets Theory To Behavioral Finance PDFDocument60 pagesFrom Ef Cient Markets Theory To Behavioral Finance PDFReluxy1No ratings yet
- English Law Week 2017: The Law - A Noble Profession or Just Business?Document32 pagesEnglish Law Week 2017: The Law - A Noble Profession or Just Business?Zviagin & CoNo ratings yet
- People vs. Santocildes Y. SigaanDocument3 pagesPeople vs. Santocildes Y. SigaanLaila Ismael SalisaNo ratings yet
- 5 Tips For Effective Resume ScreeningDocument2 pages5 Tips For Effective Resume ScreeningEmonics LLCNo ratings yet
- AoS Skaven Warscroll Card Plague MonksDocument1 pageAoS Skaven Warscroll Card Plague MonksEsh BleakeNo ratings yet
- CESMM3Document120 pagesCESMM3amiruser100% (2)
- RRLDocument3 pagesRRLFrancis Calubayan100% (1)