You might also like
- (Hand Clinics) - Pediatric Fractures Dislocations and Sequelae. Vol 22 1 Feb (2006)Document135 pages(Hand Clinics) - Pediatric Fractures Dislocations and Sequelae. Vol 22 1 Feb (2006)Bara ZsoltNo ratings yet
- Traumatic Hip Dislocations in Children and Adolescents: Pitfalls and ComplicationsDocument7 pagesTraumatic Hip Dislocations in Children and Adolescents: Pitfalls and ComplicationsFadhli Aufar KasyfiNo ratings yet
- Common Upper Limb Injuries in ChildhoodDocument9 pagesCommon Upper Limb Injuries in ChildhoodCoolnecNo ratings yet
- Fractures in ChildrenDocument9 pagesFractures in ChildrenNaylor AlubiNo ratings yet
- Frequently Missed Fractures in Pediatric TraumaDocument13 pagesFrequently Missed Fractures in Pediatric Traumaalejasuarez248No ratings yet
- Ankle Fractures in ChildrenDocument11 pagesAnkle Fractures in Childrenpafal14100% (1)
- Fracturas de Tobillo en Niños JBJS 2012Document11 pagesFracturas de Tobillo en Niños JBJS 2012Alejandro Godoy SaidNo ratings yet
- Salter Chapter XVIDocument15 pagesSalter Chapter XVISamuel Pola Karta SembiringNo ratings yet
- Basic Types of Bone FracturesDocument7 pagesBasic Types of Bone FracturesOmar Christian TuazonNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportspecheniqNo ratings yet
- Genu ValgoDocument9 pagesGenu Valgoazulqaidah95No ratings yet
- Foot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Document15 pagesFoot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Biblioteca Centro Médico De Mar del PlataNo ratings yet
- High Dislocation of the Hip Treated with Subtrochanter Femoral Shortening Osteotomy Fixed with TBWDocument7 pagesHigh Dislocation of the Hip Treated with Subtrochanter Femoral Shortening Osteotomy Fixed with TBWReza Devianto HambaliNo ratings yet
- Clavicle FractureDocument5 pagesClavicle FractureHasrul MuslihNo ratings yet
- Fractures of The Tibial PlafondDocument21 pagesFractures of The Tibial PlafondCamila FontechaNo ratings yet
- Distal Radius Fractures in AdultsDocument35 pagesDistal Radius Fractures in AdultsNicolás OpazoNo ratings yet
- Growth Plate InjuriesDocument10 pagesGrowth Plate InjuriesraissanindyaNo ratings yet
- Pediatrics FracturesDocument14 pagesPediatrics Fracturesخالد الغامديNo ratings yet
- Gaughan 2017Document12 pagesGaughan 2017Milene CamargoNo ratings yet
- Manejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementDocument9 pagesManejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementSergio Tomas Cortés MoralesNo ratings yet
- Femoral Shaft FractureDocument5 pagesFemoral Shaft FracturePrimrose Gale ParingitNo ratings yet
- Upper Extremity Injuries in Youth Sports: Jorge E. Go Mez, MS, MDDocument34 pagesUpper Extremity Injuries in Youth Sports: Jorge E. Go Mez, MS, MDАлексNo ratings yet
- Salter Chapter XVDocument16 pagesSalter Chapter XVSamuel Pola Karta SembiringNo ratings yet
- Pediatric Pelvic Fractures: Areview Article and A Case ReportDocument10 pagesPediatric Pelvic Fractures: Areview Article and A Case ReportIJAR JOURNALNo ratings yet
- Pediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorDocument7 pagesPediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorBison_sonNo ratings yet
- Traumatic Anterior Hip Dislocation in A 12-Year-Old ChildDocument3 pagesTraumatic Anterior Hip Dislocation in A 12-Year-Old ChildMikael AngelooNo ratings yet
- Ankle and Foot Injuries in The Young AthleteDocument14 pagesAnkle and Foot Injuries in The Young AthleteWalaa EldesoukeyNo ratings yet
- Tibia and Fibula Shaft Fracture in Pediatric Case (Ola)Document20 pagesTibia and Fibula Shaft Fracture in Pediatric Case (Ola)Junarto Putra Tandiarrang100% (1)
- Tompkins, JPOSNA ARTICLE 172 - FINAL UPDATEDDocument13 pagesTompkins, JPOSNA ARTICLE 172 - FINAL UPDATEDTania RahamanNo ratings yet
- Treating Stiff Elbow Joint: Causes, Diagnosis, Management"TITLE"Elbow Stiffness Treatment: Extrinsic, Intrinsic, Mixed CausesDocument8 pagesTreating Stiff Elbow Joint: Causes, Diagnosis, Management"TITLE"Elbow Stiffness Treatment: Extrinsic, Intrinsic, Mixed CausesPrabath ChinthakaNo ratings yet
- Pediatric Ankle SprainDocument8 pagesPediatric Ankle Sprainwalaa eldesoukeyNo ratings yet
- FxClavícula PDFDocument7 pagesFxClavícula PDFPenélope CrespoNo ratings yet
- Management of Pediatric Mandible Fractures PDFDocument16 pagesManagement of Pediatric Mandible Fractures PDFarfahNo ratings yet
- 2006 Trauma Self-Assessment ExaminationDocument55 pages2006 Trauma Self-Assessment ExaminationHéctor Pando SánchezNo ratings yet
- Acute and Chronic Instability of The Elbow: Bernard F. Morrey, MDDocument12 pagesAcute and Chronic Instability of The Elbow: Bernard F. Morrey, MDFadhli Aufar KasyfiNo ratings yet
- Soal TraumaDocument10 pagesSoal TraumaYoga PribadiNo ratings yet
- 3-Fracture 1Document36 pages3-Fracture 1Radwa TalaatNo ratings yet
- Acetabular Dysplasia in Adults - JBJSDocument3 pagesAcetabular Dysplasia in Adults - JBJSErnesto Ewertz MiquelNo ratings yet
- Progression and Correction of Deformities in Adults with Cerebral PalsyDocument4 pagesProgression and Correction of Deformities in Adults with Cerebral PalsyAirika PeningNo ratings yet
- Paediatric OrthopaedicDocument77 pagesPaediatric Orthopaedicdr_asalehNo ratings yet
- Common Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauDocument7 pagesCommon Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauFino SopianNo ratings yet
- Clavicle Fractures - StatPearls - NCBI BookshelfDocument9 pagesClavicle Fractures - StatPearls - NCBI BookshelfRizqan Fahlevvi AkbarNo ratings yet
- Traumatic Hip Dislocation: A ReviewDocument6 pagesTraumatic Hip Dislocation: A ReviewAna HurtadoNo ratings yet
- Disorders of The Sternoclavicular Joint: SoulderDocument14 pagesDisorders of The Sternoclavicular Joint: SoulderFillipe AgraNo ratings yet
- Care StudyDocument27 pagesCare StudyFavourNo ratings yet
- Lower Limb Deformity in ChildrenDocument13 pagesLower Limb Deformity in ChildrenShyra RahmnNo ratings yet
- Bowing Fracture Translate 2Document2 pagesBowing Fracture Translate 2yusransaadNo ratings yet
- Fractures of Thetibial PlafondDocument21 pagesFractures of Thetibial PlafondMario Esteban Muñoz RojasNo ratings yet
- Femoral Neck FractureDocument19 pagesFemoral Neck FractureTabita P SNo ratings yet
- Fracturas de Tobillo PediatricasDocument14 pagesFracturas de Tobillo PediatricasEduardo RamosNo ratings yet
- Evolution in Management of Tibial Pilon FracturesDocument9 pagesEvolution in Management of Tibial Pilon FracturestripodegrandeNo ratings yet
- Ntroduction: (1) (2) (3) Go ToDocument8 pagesNtroduction: (1) (2) (3) Go ToCoass Pediatri FKUHONo ratings yet
- Trauma - Intertrochanteric Fracture - RustiniDocument7 pagesTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08No ratings yet
- Physeal Arrest of The Distal Radius: Review ArticleDocument9 pagesPhyseal Arrest of The Distal Radius: Review ArticleAna Xiomara Cortés100% (1)
- Osteotomias PediatriaDocument13 pagesOsteotomias PediatriaM Ram CrraNo ratings yet
- GaleazziDocument11 pagesGaleazzijuanitiusNo ratings yet
- Ac Joint Seperation Clavicle FractureDocument5 pagesAc Joint Seperation Clavicle Fractureapi-356829966No ratings yet
- Giant-Cell Tumor of Bone (GCT) Is Bone Primary Tumor That Usually Happen in Young Adult Between 20-40 Years OldDocument6 pagesGiant-Cell Tumor of Bone (GCT) Is Bone Primary Tumor That Usually Happen in Young Adult Between 20-40 Years OldIbm IbamNo ratings yet
- General Principles of Fracture ManagementDocument12 pagesGeneral Principles of Fracture ManagementRita ValenteNo ratings yet
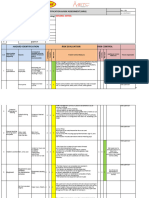
- Decking Risk AssessmentDocument4 pagesDecking Risk AssessmentReagan MukeboNo ratings yet
- Fractures of The Hallux in ChildrenDocument4 pagesFractures of The Hallux in ChildrenEdina VacariuNo ratings yet
- Acute and Chronic Humeral Shaft Fractures in Adults: SciencedirectDocument9 pagesAcute and Chronic Humeral Shaft Fractures in Adults: SciencedirectAshish AgrawalNo ratings yet
- Cramps: Follow The Instructions For R.I.C.EDocument4 pagesCramps: Follow The Instructions For R.I.C.EKenkoi SanchezNo ratings yet
- Principles of FracturesDocument34 pagesPrinciples of FracturesFabian136No ratings yet
- Sports Safety ProtocolDocument25 pagesSports Safety ProtocolHarold The GreatNo ratings yet
- Inter and Sub Trochanteric FractureDocument25 pagesInter and Sub Trochanteric Fracturedevi shree100% (1)
- What Are The Different Types of Traction?Document5 pagesWhat Are The Different Types of Traction?keithevaristoNo ratings yet
- Fracture Ayurveda Managaement (Bhagna)Document48 pagesFracture Ayurveda Managaement (Bhagna)drhemantt1099100% (3)
- Orthopedic Trauma: Assessment and Care: 2 Contact Hours Course Expires: April 30, 2018Document34 pagesOrthopedic Trauma: Assessment and Care: 2 Contact Hours Course Expires: April 30, 2018najibNo ratings yet
- Casting Techniques PDFDocument14 pagesCasting Techniques PDFVasanth Kumar AllaNo ratings yet
- Physical Therapy Toolkit ™: 66 Treatment Guides 211 HandoutsDocument4 pagesPhysical Therapy Toolkit ™: 66 Treatment Guides 211 HandoutsKiné Therapeut-manuelle Masseur GabiNo ratings yet
- Musculoskeletal MED SURGDocument57 pagesMusculoskeletal MED SURGlolo0880No ratings yet
- FRACTUREDocument16 pagesFRACTUREPriyaNo ratings yet
- My Seminar-Fracture of The MandibleDocument25 pagesMy Seminar-Fracture of The MandibleKhalid Mahmud Arifin100% (36)
- Musculoskeletal Radiology NotesDocument62 pagesMusculoskeletal Radiology Notesmeshmatic1234567100% (3)
- Management of Mandibular Angle FractureDocument10 pagesManagement of Mandibular Angle FractureRudnapon AmornlaksananonNo ratings yet
- First Aid AssignmentDocument10 pagesFirst Aid AssignmentmusajamesNo ratings yet
- LESSON PLAN ON FRACTUREDocument27 pagesLESSON PLAN ON FRACTUREVaishali Singh100% (1)
- AxSOS 13Document28 pagesAxSOS 13Dan IonescuNo ratings yet
- FracturesDocument18 pagesFracturesNicole Anne ValerioNo ratings yet
- Surgical Extraction of The Impacted Mandibular Third MolarDocument84 pagesSurgical Extraction of The Impacted Mandibular Third MolarShalini Thakur Dubey100% (9)
- TARGET 200 PLUS Orthopaedics GuideDocument21 pagesTARGET 200 PLUS Orthopaedics GuideTMC PGI GENER MICKONo ratings yet
- Early Versus Delayed Surgery For Paediatric Supracondylar Humeral Fractures in The Absence of Vascular CompromiseDocument7 pagesEarly Versus Delayed Surgery For Paediatric Supracondylar Humeral Fractures in The Absence of Vascular CompromiseindrayudhaaNo ratings yet
- GALEAZZI AND MONTEGGIA FRACTURE CAREDocument31 pagesGALEAZZI AND MONTEGGIA FRACTURE CAREnihthaNo ratings yet
- Fractured Thumb 5Document20 pagesFractured Thumb 5Noor Al Zahraa AliNo ratings yet
- Trochanteric Buttress PlateDocument13 pagesTrochanteric Buttress PlateAshutNo ratings yet
- Clasificacion AO 2007Document162 pagesClasificacion AO 2007Aliz VargasNo ratings yet
- Management of Distal Radius Fractures - Treatment Protocol and Functional ResultsDocument7 pagesManagement of Distal Radius Fractures - Treatment Protocol and Functional Resultslex salomNo ratings yet
- Fundamentals of Skeletal RadiologyDocument247 pagesFundamentals of Skeletal Radiologymihaela2786100% (1)