You might also like
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementFrom EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNo ratings yet
- Medicine: Allopurinol Use and Type 2 Diabetes Incidence Among Patients With GoutDocument7 pagesMedicine: Allopurinol Use and Type 2 Diabetes Incidence Among Patients With GoutGrady CoolNo ratings yet
- ResponseConsensusReportAntipsychoticsMetabolicIssuesLetter CITROME DiabCare2004Document5 pagesResponseConsensusReportAntipsychoticsMetabolicIssuesLetter CITROME DiabCare2004Leslie CitromeNo ratings yet
- The Efficacy of Okra (Abelmoschus Esculentus) in Decreasing Blood Sugar Levels Among Patients With Impaired Fasting Glucose in Antipolo CityDocument4 pagesThe Efficacy of Okra (Abelmoschus Esculentus) in Decreasing Blood Sugar Levels Among Patients With Impaired Fasting Glucose in Antipolo CityMa. Isabel AzañaNo ratings yet
- Medication-Induced Diabetes MellitusDocument6 pagesMedication-Induced Diabetes MellitusAmjadNo ratings yet
- RosperidonDocument7 pagesRosperidonEndang SusilowatiNo ratings yet
- Renal and Retinal Effects of Enalapril and Losartan in Type 1 DiabetesDocument12 pagesRenal and Retinal Effects of Enalapril and Losartan in Type 1 DiabetesDina Malisa Nugraha, MDNo ratings yet
- FDA AnalysisDocument7 pagesFDA AnalysisRidha Surya NugrahaNo ratings yet
- Journal 1 Nejmoa1506930Document11 pagesJournal 1 Nejmoa1506930Dyo O RNo ratings yet
- 2 DyslipidemiaDocument7 pages2 DyslipidemiaShengyou ZengNo ratings yet
- Prader-Willy Fda OzempicDocument16 pagesPrader-Willy Fda OzempicJailza MartinsNo ratings yet
- Geographic and Clinical Variation in Clozapine Use in The United StatesDocument7 pagesGeographic and Clinical Variation in Clozapine Use in The United StatesEvaG2012No ratings yet
- Retinopathy DiabeticDocument5 pagesRetinopathy DiabeticMagnaNo ratings yet
- Psychopharmacologictreatment Ofpsychosisinchildrenand AdolescentsDocument18 pagesPsychopharmacologictreatment Ofpsychosisinchildrenand AdolescentsbogdancoticaNo ratings yet
- DEPICT 1 - T1D StudyDocument13 pagesDEPICT 1 - T1D StudyGVRNo ratings yet
- PCOS and Metabolic SyndromeDocument21 pagesPCOS and Metabolic SyndromeHAVIZ YUADNo ratings yet
- Righi (2016)Document6 pagesRighi (2016)PelagyalNo ratings yet
- Weight Loss Drug Cutting Risk of Heart AttackDocument12 pagesWeight Loss Drug Cutting Risk of Heart AttackWKYC.comNo ratings yet
- Semaglutide and Cardiovascular Outcomes in Obesity Without DiabetesDocument12 pagesSemaglutide and Cardiovascular Outcomes in Obesity Without Diabetesmengyanli.528No ratings yet
- Igweokpala, 2023Document11 pagesIgweokpala, 2023Mirilláiny AnacletoNo ratings yet
- Chap 1Document3 pagesChap 1Samreen JawaidNo ratings yet
- The Pubertal Presentation of Polycystic Ovary Syndrome PCOS 2002 Fertility and SterilityDocument1 pageThe Pubertal Presentation of Polycystic Ovary Syndrome PCOS 2002 Fertility and SterilityfujimeisterNo ratings yet
- Pioglitazone After Ischemic Stroke or Transient Ischemic AttackDocument11 pagesPioglitazone After Ischemic Stroke or Transient Ischemic AttackBiola DwikoNo ratings yet
- Lipid Lowering DrugsDocument2 pagesLipid Lowering DrugsstambicaNo ratings yet
- Literature Review EscitalopramDocument6 pagesLiterature Review Escitalopramc5swkkcn100% (1)
- Nonalcoholic SteatohepatitisDocument15 pagesNonalcoholic SteatohepatitisLucas VenturaNo ratings yet
- Medip, IJCP-2856 ODocument6 pagesMedip, IJCP-2856 OMarcelita DuwiriNo ratings yet
- ASCP Corner Increased Risk of Cerebrovascular Adverse Events and Death in Elderly Demented PatienDocument1 pageASCP Corner Increased Risk of Cerebrovascular Adverse Events and Death in Elderly Demented PatienSantosh KumarNo ratings yet
- SPW Diazoxide CholinDocument10 pagesSPW Diazoxide CholinlailagsazNo ratings yet
- Potent Antihypertensive Action of Dietary Flaxseed in Hypertensive PatientsDocument13 pagesPotent Antihypertensive Action of Dietary Flaxseed in Hypertensive PatientsMaRiana TorresNo ratings yet
- Use of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaDocument4 pagesUse of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaPutu Agus GrantikaNo ratings yet
- Effect of Chlorpromazine and Haloperidol Combination on Lipid LevelsDocument10 pagesEffect of Chlorpromazine and Haloperidol Combination on Lipid LevelstrianaamaliaNo ratings yet
- Revista Medica ChilenaDocument10 pagesRevista Medica ChilenaMayita DurNo ratings yet
- High-Intensity Statins Are Associated With Increased Incidence of Hypoglycemia During Hospitalization of Individuals Not Critically IllDocument6 pagesHigh-Intensity Statins Are Associated With Increased Incidence of Hypoglycemia During Hospitalization of Individuals Not Critically IllNermine S. ChoumanNo ratings yet
- Donepezil in Vascular Dementia: A Randomized, Placebo-Controlled StudyDocument9 pagesDonepezil in Vascular Dementia: A Randomized, Placebo-Controlled StudyDian ArdiansyahNo ratings yet
- Gebhardt2007 Article ClozapineOlanzapine-InducedRecDocument5 pagesGebhardt2007 Article ClozapineOlanzapine-InducedRecrossibNo ratings yet
- Bauch-Atrial Natriuretic Peptide As A MarDocument6 pagesBauch-Atrial Natriuretic Peptide As A MarSzendeNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- Clinical Course of Diabetic Ketoacidosis in Hypertriglyceridemic Pancreatitis Pancreas 2015Document4 pagesClinical Course of Diabetic Ketoacidosis in Hypertriglyceridemic Pancreatitis Pancreas 2015América FloresNo ratings yet
- Jama Slomski 2021 JN 210028 1637771580.15064Document1 pageJama Slomski 2021 JN 210028 1637771580.15064Luis Adrian Rivera PomalesNo ratings yet
- Tsuyuki 2002Document7 pagesTsuyuki 2002Basilharbi HammadNo ratings yet
- Whats New of PcosDocument9 pagesWhats New of PcosbambangNo ratings yet
- Hormone Therapy in Postmenopausal WomenDocument8 pagesHormone Therapy in Postmenopausal WomenChyntia Pramita SariNo ratings yet
- Focus On The Clinical Ramifications of Antipsychotic Choice For The Risk For Developing Type 2 Diabetes MellitusDocument5 pagesFocus On The Clinical Ramifications of Antipsychotic Choice For The Risk For Developing Type 2 Diabetes MellitusLeslie CitromeNo ratings yet
- Funcion RenalDocument11 pagesFuncion RenalCarlos AvalosNo ratings yet
- Addition of Dipeptidyl Peptidase-4 Inhibitors To Sulphonylureas and Risk of Hypoglycaemia: Systematic Review and Meta-AnalysisDocument9 pagesAddition of Dipeptidyl Peptidase-4 Inhibitors To Sulphonylureas and Risk of Hypoglycaemia: Systematic Review and Meta-AnalysisEmanuel BaltigNo ratings yet
- Emailing Expression of KGF-1 and KGF-2 in Skin Wounds ADocument12 pagesEmailing Expression of KGF-1 and KGF-2 in Skin Wounds ARimaWulansariNo ratings yet
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesDocument12 pagesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesMoeez AkramNo ratings yet
- Eria 2Document11 pagesEria 2ruth angelinaNo ratings yet
- Ajp.161.10.1837 2Document11 pagesAjp.161.10.1837 2HKANo ratings yet
- Hypoglycemia - 2014 Morales N DoronDocument8 pagesHypoglycemia - 2014 Morales N DoronDian Eka RamadhaniNo ratings yet
- P 007 OlanzapineDocument11 pagesP 007 OlanzapineBalasubrahmanya K. R.No ratings yet
- Lo Per Amide Therapy For Acute Diarrhea in Children Systematic Review and Meta-AnalysisDocument11 pagesLo Per Amide Therapy For Acute Diarrhea in Children Systematic Review and Meta-AnalysisAprilia R. PermatasariNo ratings yet
- Knowledge Gap in DiabetesDocument3 pagesKnowledge Gap in Diabetesamit545No ratings yet
- Soal PG Endokrin MahasiswaDocument5 pagesSoal PG Endokrin MahasiswaSandwingNo ratings yet
- 23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25Document5 pages23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25observacionfray23No ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Platelet Activating FactorDocument8 pagesPlatelet Activating FactorayesayeziaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
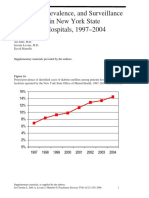
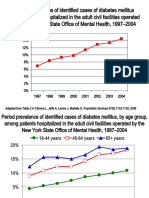
- Incidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Document5 pagesIncidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Leslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- Diabetes prevalence trends in NY mental hospitalsDocument8 pagesDiabetes prevalence trends in NY mental hospitalsLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- NR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaDocument1 pageNR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaLeslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- INTRODUCTION (Continued)Document1 pageINTRODUCTION (Continued)Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- Ziprasidone efficacy against hostility in schizophreniaDocument1 pageZiprasidone efficacy against hostility in schizophreniaLeslie CitromeNo ratings yet
- Catechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsDocument3 pagesCatechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsLeslie CitromeNo ratings yet
- ReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Document1 pageReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- QuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Document1 pageQuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- Drug StudyDocument7 pagesDrug StudyJohn Paulo MataNo ratings yet
- Schizophrenia and Other Psychotic Disorders Clinical Practice GuidelineDocument7 pagesSchizophrenia and Other Psychotic Disorders Clinical Practice GuidelineDani NugrohoNo ratings yet
- Comprehensive Neurology Board Review-THIRD EDITIONDocument44 pagesComprehensive Neurology Board Review-THIRD EDITIONDr. Chaim B. Colen50% (4)
- Assessment and Emergency Management of The Acutely Agitated or Violent Adult - UpToDateDocument20 pagesAssessment and Emergency Management of The Acutely Agitated or Violent Adult - UpToDateImja94100% (1)
- Schizophrenia Treatment & ManagementDocument16 pagesSchizophrenia Treatment & ManagementDimas Januar100% (2)
- Tehreem - Recalls MODIFIED BY Me & AARAVDocument58 pagesTehreem - Recalls MODIFIED BY Me & AARAVRohini SelvarajahNo ratings yet
- GNC Psy Nursing QuestionsDocument34 pagesGNC Psy Nursing QuestionsFan Eli100% (1)
- Antipsychotic Drugs Grandiosity Hallucinations Paranoia DelusionsDocument63 pagesAntipsychotic Drugs Grandiosity Hallucinations Paranoia DelusionsMuhammad Masoom Akhtar100% (1)
- 1.schizophrenia An Overview PDFDocument5 pages1.schizophrenia An Overview PDFNadyaNo ratings yet
- Injection SOP 2011 (3rd Edition)Document70 pagesInjection SOP 2011 (3rd Edition)lynlgsxrNo ratings yet
- SchizophreniaDocument7 pagesSchizophreniaMANOJ KUMARNo ratings yet
- Schizophrenia Guide EN PDFDocument79 pagesSchizophrenia Guide EN PDFMichaelus1No ratings yet
- First Generation AntipsychoticDocument4 pagesFirst Generation AntipsychoticPutu Agus Grantika100% (1)
- Psychopharmacology in PsychiatryDocument94 pagesPsychopharmacology in PsychiatryOslo SaputraNo ratings yet
- Third Generation Antipsychotic DrugsDocument45 pagesThird Generation Antipsychotic DrugsGabriela Drima100% (1)
- Antipsychotic: Antipsychotics, Also Known As NeurolepticsDocument28 pagesAntipsychotic: Antipsychotics, Also Known As NeurolepticsJussel Vazquez MarquezNo ratings yet
- Drug Study 2019Document14 pagesDrug Study 2019Aubrey Unique Evangelista100% (1)
- Extrapyramidal Symptoms Guide: Dystonia, Akathisia, Parkinsonism & Tardive DyskinesiaDocument35 pagesExtrapyramidal Symptoms Guide: Dystonia, Akathisia, Parkinsonism & Tardive DyskinesiaLucas PhiNo ratings yet
- Handbook of Psychiatric Drugs 08 PDFDocument275 pagesHandbook of Psychiatric Drugs 08 PDFlucian_vatamanu100% (3)
- Schizophrenia Diagnosis, Symptoms & Treatment /TITLEDocument50 pagesSchizophrenia Diagnosis, Symptoms & Treatment /TITLEelvinegunawanNo ratings yet
- Psychopharmacological AgentsDocument44 pagesPsychopharmacological Agentsbazet49No ratings yet
- Neuroleptics & AnxiolyticsDocument65 pagesNeuroleptics & AnxiolyticsAntonPurpurovNo ratings yet
- Perspectives in Pharmacology: Roger D. Porsolt, Vincent Castagné, Eric Hayes, and David VirleyDocument5 pagesPerspectives in Pharmacology: Roger D. Porsolt, Vincent Castagné, Eric Hayes, and David Virleyel egendNo ratings yet
- Abnormal Psychology 2nd Edition Nolen-Hoeksema Test Bank 1Document52 pagesAbnormal Psychology 2nd Edition Nolen-Hoeksema Test Bank 1jamie100% (31)
- Psychotropic Medications During PregnancyDocument20 pagesPsychotropic Medications During PregnancyMaria Von ShaftNo ratings yet
- 2018 Article 1999 PDFDocument8 pages2018 Article 1999 PDFyusma haranisNo ratings yet
- Antipsychotic Drugs: Presentation By-Sumaiya SadafDocument19 pagesAntipsychotic Drugs: Presentation By-Sumaiya SadafSweta ShahNo ratings yet
- Archives of Clinical Psychiatry - R de Psiquiatria - Vol. 47 - 6 - 2020Document63 pagesArchives of Clinical Psychiatry - R de Psiquiatria - Vol. 47 - 6 - 2020Danilo Pereira GonçalvesNo ratings yet
- Which Drugs Can Cause Neuroleptic Malignant Syndrome?: Medicines Q&AsDocument6 pagesWhich Drugs Can Cause Neuroleptic Malignant Syndrome?: Medicines Q&AsLaily MasrurohNo ratings yet