You might also like
- Combining CBT and Medication: An Evidence-Based ApproachFrom EverandCombining CBT and Medication: An Evidence-Based ApproachRating: 3 out of 5 stars3/5 (1)
- Self-assessment Questions for Clinical Molecular GeneticsFrom EverandSelf-assessment Questions for Clinical Molecular GeneticsRating: 5 out of 5 stars5/5 (1)
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Verbal De-Escalation Agitated PatientDocument9 pagesVerbal De-Escalation Agitated PatientArhip CojocNo ratings yet
- MedEdicus Insomnia CME and Test Questions PDFDocument20 pagesMedEdicus Insomnia CME and Test Questions PDFmeiutaNo ratings yet
- Cns Spectrums: The Clinical Challenges of Akathisia CME Review ArticleDocument16 pagesCns Spectrums: The Clinical Challenges of Akathisia CME Review Articledzakiyah nurul israNo ratings yet
- A Case for Looking: Bridging the Technical and the SpiritualFrom EverandA Case for Looking: Bridging the Technical and the SpiritualNo ratings yet
- Contemporary Psychiatric Mental Health Nursing 3rd Edition Kneisl Solutions ManualDocument13 pagesContemporary Psychiatric Mental Health Nursing 3rd Edition Kneisl Solutions Manualphenicboxironicu9100% (26)
- Learned Mindfulness: Physician Engagement and M.D. WellnessFrom EverandLearned Mindfulness: Physician Engagement and M.D. WellnessNo ratings yet
- Strategies To Improve Medication Adherence in Patients With Schizophrenia: The Role of Support ServicesDocument15 pagesStrategies To Improve Medication Adherence in Patients With Schizophrenia: The Role of Support ServicesSatrio WibowoNo ratings yet
- Principle-Based Stepped Care and Brief Psychotherapy for Integrated Care SettingsFrom EverandPrinciple-Based Stepped Care and Brief Psychotherapy for Integrated Care SettingsAlexandros MaragakisNo ratings yet
- How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyDocument17 pagesHow Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyAlexNo ratings yet
- Conceptual Framework To Support Service Intervention Model On The Outcome of Drug Compliance and Psychological Well-Being Among Patients With Mental DisordersDocument3 pagesConceptual Framework To Support Service Intervention Model On The Outcome of Drug Compliance and Psychological Well-Being Among Patients With Mental DisordersMalarvizhi SureshNo ratings yet
- Stubbs - Merrill 2019 Addiction Disorder Considerations For Patients Seeking Psychotherapy Icns - 16Document5 pagesStubbs - Merrill 2019 Addiction Disorder Considerations For Patients Seeking Psychotherapy Icns - 16xqiekupdcvjnqgjugkNo ratings yet
- De-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Document4 pagesDe-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Urgencias HorwitzNo ratings yet
- Update On ART-2010Document30 pagesUpdate On ART-2010danayanto sumbungNo ratings yet
- Textbook of Clinical Nutrition and Functional Medicine, vol. 2: Protocols for Common Inflammatory DisordersFrom EverandTextbook of Clinical Nutrition and Functional Medicine, vol. 2: Protocols for Common Inflammatory DisordersRating: 4 out of 5 stars4/5 (1)
- Mindfulness-Based Treatment Approaches: Clinician's Guide to Evidence Base and ApplicationsFrom EverandMindfulness-Based Treatment Approaches: Clinician's Guide to Evidence Base and ApplicationsRating: 4 out of 5 stars4/5 (2)
- Chapter 036Document16 pagesChapter 036dtheart2821100% (4)
- Scholarly PaperDocument5 pagesScholarly Paperapi-662219485No ratings yet
- Management of Allergic Reactions and Anaphylaxis in The EmergencyDocument23 pagesManagement of Allergic Reactions and Anaphylaxis in The EmergencyAna Belén Viteri luzuriagaNo ratings yet
- Journey to Healing: The Art and Science of Applied KinesiologyFrom EverandJourney to Healing: The Art and Science of Applied KinesiologyNo ratings yet
- Practice Guideline For The Treatment of Patients With Obsessive-Compulsive DisorderDocument117 pagesPractice Guideline For The Treatment of Patients With Obsessive-Compulsive DisorderBeatriz LavorNo ratings yet
- JaffeDocument2 pagesJafferbtakemotoNo ratings yet
- PICOTDocument8 pagesPICOTRaphael Seke OkokoNo ratings yet
- Opioid Analgesics: Symposium On Pain MedicineDocument12 pagesOpioid Analgesics: Symposium On Pain Medicineyunica simanjuntakNo ratings yet
- Aisha Isyaku Term PaperDocument27 pagesAisha Isyaku Term PaperUsman Ahmad TijjaniNo ratings yet
- Clinical Nursing JudgementDocument5 pagesClinical Nursing Judgementapi-546503916No ratings yet
- Anti-Aging Therapeutics Volume XIIIFrom EverandAnti-Aging Therapeutics Volume XIIINo ratings yet
- Treatment-Resistant Mood Disorders (Oxford Psychiatry Library) (PDFDrive)Document175 pagesTreatment-Resistant Mood Disorders (Oxford Psychiatry Library) (PDFDrive)elidy_1No ratings yet
- Pharmacology Unit 2Document19 pagesPharmacology Unit 2Bea Bianca CruzNo ratings yet
- Motivational IntervieweDocument20 pagesMotivational IntervieweKedai GelutNo ratings yet
- Board Review in Preventive Medicine and Public HealthFrom EverandBoard Review in Preventive Medicine and Public HealthRating: 3.5 out of 5 stars3.5/5 (2)
- Patterns of Psychologists Interprofessional Collaboration AcrossDocument26 pagesPatterns of Psychologists Interprofessional Collaboration AcrossLNNGANo ratings yet
- PrintVersion PDFDocument28 pagesPrintVersion PDFUswaPutriemelelaNo ratings yet
- Textbook of Clinical Nutrition and Functional Medicine, vol. 1: Essential Knowledge for Safe Action and Effective TreatmentFrom EverandTextbook of Clinical Nutrition and Functional Medicine, vol. 1: Essential Knowledge for Safe Action and Effective TreatmentNo ratings yet
- Healthcare ProcessDocument40 pagesHealthcare ProcessSJO1 G6- Escaro,Shaira JoyNo ratings yet
- Integrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionFrom EverandIntegrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionNo ratings yet
- Basic Nursing PharmacologyDocument78 pagesBasic Nursing PharmacologyLloyd Rafael EstabilloNo ratings yet
- Therapist's Guide to Posttraumatic Stress Disorder InterventionFrom EverandTherapist's Guide to Posttraumatic Stress Disorder InterventionNo ratings yet
- Danhauer 2017 Reviewof Yoga Therapy During Cancer TreatmentDocument24 pagesDanhauer 2017 Reviewof Yoga Therapy During Cancer TreatmentfitranoenoeNo ratings yet
- Joaquín Andrade & David Feinstein - ENERGY PSYCHOLOGYDocument19 pagesJoaquín Andrade & David Feinstein - ENERGY PSYCHOLOGYlandburender100% (1)
- Migraine: Emerging Innovations and Treatment OptionsFrom EverandMigraine: Emerging Innovations and Treatment OptionsShalini ShahNo ratings yet
- Evidence-Based Practice in Pediatric Physical Therapy by BarryDocument14 pagesEvidence-Based Practice in Pediatric Physical Therapy by BarryFe TusNo ratings yet
- Evidence-Based Evaluation & Management of Common Spinal Conditions: A Guide for the Manual PractitionerFrom EverandEvidence-Based Evaluation & Management of Common Spinal Conditions: A Guide for the Manual PractitionerRating: 5 out of 5 stars5/5 (1)
- Self Management in Pediatric Inflammatory Bowel.24Document8 pagesSelf Management in Pediatric Inflammatory Bowel.24Lizette MirandaNo ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Essential Physical Therapy Terminology: Navigating Physical Therapy LanguageFrom EverandEssential Physical Therapy Terminology: Navigating Physical Therapy LanguageNo ratings yet
- Exam 1 (NUR-152)Document5 pagesExam 1 (NUR-152)davidvpnNo ratings yet
- Prof. DR - Manal Hamed: Prepared byDocument26 pagesProf. DR - Manal Hamed: Prepared byM EhabNo ratings yet
- Transformative Health Strategies: Integrative Medicine and the COVID-19 PandemicFrom EverandTransformative Health Strategies: Integrative Medicine and the COVID-19 PandemicNo ratings yet
- BUTALON Assessment 1Document7 pagesBUTALON Assessment 1Kc Cassandra ButalonNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
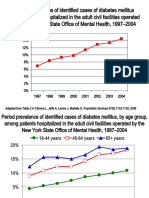
- DiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Document8 pagesDiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Leslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Leslie CitromeNo ratings yet
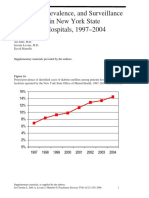
- DiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineDocument5 pagesDiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- ZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Document1 pageZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Leslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Leslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- Leslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDDocument1 pageLeslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDLeslie CitromeNo ratings yet
- MoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Document1 pageMoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- DivalproexDRtoERClinicalTrialAPA Poster CITROME APA2004Document1 pageDivalproexDRtoERClinicalTrialAPA Poster CITROME APA2004Leslie CitromeNo ratings yet
- Mood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Document1 pageMood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Leslie CitromeNo ratings yet
- DosingSGAPosterWCBPHandout CITROME 2005Document4 pagesDosingSGAPosterWCBPHandout CITROME 2005Leslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Leslie CitromeNo ratings yet
- NewTreatmentsAgitationReview CITROME PsychQuarterly2004Document18 pagesNewTreatmentsAgitationReview CITROME PsychQuarterly2004Leslie CitromeNo ratings yet
- Material 1 (Writing Good Upwork Proposals)Document3 pagesMaterial 1 (Writing Good Upwork Proposals)OvercomerNo ratings yet
- Allarco Alberta Statement of Claim OCR PDFDocument12 pagesAllarco Alberta Statement of Claim OCR PDFHoward KnopfNo ratings yet
- COMM294 SyllabusDocument4 pagesCOMM294 SyllabuswdorfmannNo ratings yet
- Gremlins 3Document12 pagesGremlins 3Kenny TadrzynskiNo ratings yet
- Rodriguez Pinto v. Cirilo Tirado, 1st Cir. (1993)Document27 pagesRodriguez Pinto v. Cirilo Tirado, 1st Cir. (1993)Scribd Government DocsNo ratings yet
- Anonymous Rise Up Shepherd and Follow For Violin Viola Piano 71302 PDFDocument3 pagesAnonymous Rise Up Shepherd and Follow For Violin Viola Piano 71302 PDFSt TsNo ratings yet
- Assignment 33Document4 pagesAssignment 33Imran Khan JunejoNo ratings yet
- Software Architechture Assignment - 2023MT93112Document15 pagesSoftware Architechture Assignment - 2023MT93112Adil NasimNo ratings yet
- Marcel and The White Star 1Document12 pagesMarcel and The White Star 1Ali Hamidi100% (1)
- Socio Cultural Factors Influencing Child Nutrition Among Mothers in Calabar Municipality Cross River State NigeriaDocument34 pagesSocio Cultural Factors Influencing Child Nutrition Among Mothers in Calabar Municipality Cross River State NigeriaTAJUDEEN AZEEZNo ratings yet
- AFFIRMATIONS of LOUISE HAYDocument18 pagesAFFIRMATIONS of LOUISE HAYVRnlp91% (32)
- NSTP CM Week 6Document10 pagesNSTP CM Week 6dankmemerhuskNo ratings yet
- Exile in Dapitan (1892-1896)Document5 pagesExile in Dapitan (1892-1896)Mary Leigh TenezaNo ratings yet
- Emtech Lecture 1Document2 pagesEmtech Lecture 1Shayra VillacortaNo ratings yet
- GGplot2 TemasDocument81 pagesGGplot2 TemasmoraleseconomiaNo ratings yet
- Case Study DMDocument2 pagesCase Study DMMomina TariqNo ratings yet
- August 2012 NewsletterDocument27 pagesAugust 2012 NewsletterBiewBiewNo ratings yet
- ZooDocument73 pagesZoovijay saniNo ratings yet
- 100 + 1 Big Lies of MacedonismDocument158 pages100 + 1 Big Lies of MacedonismJames PetersonNo ratings yet
- Bezza SST 010722Document1 pageBezza SST 010722Rachel LeeNo ratings yet
- Physical Hazards 101Document24 pagesPhysical Hazards 101Mohamed AhmedNo ratings yet
- Food Groups and What They DoDocument26 pagesFood Groups and What They DoCesar FloresNo ratings yet
- Tomas CVDocument2 pagesTomas CVtroy2brown0% (1)
- Top Gun CUT-40MDocument9 pagesTop Gun CUT-40MTom PleysierNo ratings yet
- Comments On Manual Dexterity-NYTDocument78 pagesComments On Manual Dexterity-NYTSao LaoNo ratings yet
- Astri Yuniar Sri Utari: The Usage of Multiple Choice .: CompletionDocument11 pagesAstri Yuniar Sri Utari: The Usage of Multiple Choice .: CompletionHoàng Tạ KimNo ratings yet
- Soal Usp Bhs InggrisDocument4 pagesSoal Usp Bhs InggrisRASA RASANo ratings yet
- Second Division G.R. No. 212860, March 14, 2018 Republic of The Philippines, Petitioner, V. Florie Grace M. Cote, Respondent. Decision REYES, JR., J.Document6 pagesSecond Division G.R. No. 212860, March 14, 2018 Republic of The Philippines, Petitioner, V. Florie Grace M. Cote, Respondent. Decision REYES, JR., J.cnfhdxNo ratings yet
- Public Speaking-From Preparation To Presentation: How To Become Confident, Relaxed and MeaningfulDocument4 pagesPublic Speaking-From Preparation To Presentation: How To Become Confident, Relaxed and MeaningfulNadya KhairunaNo ratings yet
- 1 Crim1 - People Vs Javier - Lack of Intent To Commit So Grave A WrongDocument2 pages1 Crim1 - People Vs Javier - Lack of Intent To Commit So Grave A WrongJustin Reden BautistaNo ratings yet