You might also like
- Handbook of Autism and AnxietyFrom EverandHandbook of Autism and AnxietyThompson E. Davis IIINo ratings yet
- Schizophr Bull 1987 Kay 261 76Document16 pagesSchizophr Bull 1987 Kay 261 76lucicosoNo ratings yet
- Sexual Orientation and Psychodynamic Psychotherapy: Sexual Science and Clinical PracticeFrom EverandSexual Orientation and Psychodynamic Psychotherapy: Sexual Science and Clinical PracticeNo ratings yet
- Association Between Specific Childhood Adversities and Symptom Dimensions in People With Psychosis - Systematic Review and Meta-AnalysisDocument11 pagesAssociation Between Specific Childhood Adversities and Symptom Dimensions in People With Psychosis - Systematic Review and Meta-AnalysisSusana Pérez ReyesNo ratings yet
- Hwu 1997Document6 pagesHwu 1997dad dzd adaNo ratings yet
- Psychopathology in Non-Clinically Referred Sexually Abused Children - Mcleer, S. V. Et. Al.Document8 pagesPsychopathology in Non-Clinically Referred Sexually Abused Children - Mcleer, S. V. Et. Al.martiinrv100% (1)
- Anhedonia, Positive and Negative Affect, and Social Functioning in SchizophreniaDocument12 pagesAnhedonia, Positive and Negative Affect, and Social Functioning in SchizophreniaAlexis N. IbarraNo ratings yet
- In Uence of Gender On Social Outcome in SchizophreniaDocument7 pagesIn Uence of Gender On Social Outcome in SchizophreniaScheckyNo ratings yet
- Personality and Seasonal Affective Disorder: Results From The CAN-SAD StudyDocument8 pagesPersonality and Seasonal Affective Disorder: Results From The CAN-SAD Studyembi68No ratings yet
- The Relationship of Cognitive Functions and Psychopathology On The Level of Insight in Patients With SchizophreniaDocument6 pagesThe Relationship of Cognitive Functions and Psychopathology On The Level of Insight in Patients With SchizophrenianandhaNo ratings yet
- Mental HealthDocument8 pagesMental HealthJohn TelekNo ratings yet
- Somatic Symptoms in Children and Adolescents With Anxiety DisordersDocument9 pagesSomatic Symptoms in Children and Adolescents With Anxiety DisordersDũng HồNo ratings yet
- Vaskin 2009Document3 pagesVaskin 2009RosarioBengocheaSecoNo ratings yet
- The Relationship Between Schizo-Affective, Schizophrenic and Mood Disorders in Patients Admitted at Mathari Psychiatric Hospital, Nairobi, KenyaDocument8 pagesThe Relationship Between Schizo-Affective, Schizophrenic and Mood Disorders in Patients Admitted at Mathari Psychiatric Hospital, Nairobi, KenyaLunaFiaNo ratings yet
- Schizophr Bull 1987 Kay 261-76-2Document16 pagesSchizophr Bull 1987 Kay 261-76-2Anonymous hvOuCjNo ratings yet
- Altered brain activity related to social norm violations is a heritable biomarker for social anxiety disorderDocument10 pagesAltered brain activity related to social norm violations is a heritable biomarker for social anxiety disorderCanNo ratings yet
- MaturitasDocument3 pagesMaturitasCarolinaNo ratings yet
- Affective Instability and Suicidal Ideat20160629 23040 WFCGFH With Cover Page v2Document16 pagesAffective Instability and Suicidal Ideat20160629 23040 WFCGFH With Cover Page v2Clarice Almeida da SilvaNo ratings yet
- SIndrome HuntingtonDocument7 pagesSIndrome HuntingtonCrecer Con la MúsicaNo ratings yet
- The Evolution of Illness Phases in Schizophrenia A Non Parametric Item Response Analysis of The Positive and Negative Syndrome ScaleDocument37 pagesThe Evolution of Illness Phases in Schizophrenia A Non Parametric Item Response Analysis of The Positive and Negative Syndrome ScaleLasharia ClarkeNo ratings yet
- Schizo 3Document11 pagesSchizo 3Aldy GeriNo ratings yet
- Abstract Sull'Assertivita'Document45 pagesAbstract Sull'Assertivita'Gabriella Mae Magpayo ValentinNo ratings yet
- Assertiveness research abstractsDocument45 pagesAssertiveness research abstractsGabriella Mae Magpayo ValentinNo ratings yet
- Pietrzak 2013Document1 pagePietrzak 2013MikerenNo ratings yet
- The Influence of Gender On Social Anxiety Spectrum Symptoms in A Sample of University StudentsDocument7 pagesThe Influence of Gender On Social Anxiety Spectrum Symptoms in A Sample of University StudentsGeorge WinchesterNo ratings yet
- Chang 2018Document14 pagesChang 2018spaciugNo ratings yet
- Fear of Negative Evaluation, Trait Anxiety, and Judgment Bias in Adults Who StutterDocument13 pagesFear of Negative Evaluation, Trait Anxiety, and Judgment Bias in Adults Who StutterDai ArhexNo ratings yet
- Escala de AgresividadDocument6 pagesEscala de AgresividadCDBHNo ratings yet
- Evidence-Based Guideline: Assessment and Management of Psychiatric Disorders in Individuals With MSDocument9 pagesEvidence-Based Guideline: Assessment and Management of Psychiatric Disorders in Individuals With MSChon ChiNo ratings yet
- ALTERACIaN DEL LENGUAJE COMO PREDICTOR DEL INICIO DE LA PSICOSIS EN JaVENES CON RIESGO CL+NICO AUMENTADODocument2 pagesALTERACIaN DEL LENGUAJE COMO PREDICTOR DEL INICIO DE LA PSICOSIS EN JaVENES CON RIESGO CL+NICO AUMENTADOAlí Amaroo Pellicer OchoaNo ratings yet
- Anhedonia EqzDocument12 pagesAnhedonia EqzalfigebaNo ratings yet
- Psychiatry ResearchDocument7 pagesPsychiatry ResearchLetyAlarcónNo ratings yet
- Decoding Rumination A Machine Learning Approach To A Tra - 2020 - Journal of PsDocument7 pagesDecoding Rumination A Machine Learning Approach To A Tra - 2020 - Journal of PsMichael WondemuNo ratings yet
- Influence of Child Abuse On Adult Depression: Moderation by The Corticotropin-Releasing Hormone Receptor GeneDocument11 pagesInfluence of Child Abuse On Adult Depression: Moderation by The Corticotropin-Releasing Hormone Receptor GeneDian Sulistya EkaputriNo ratings yet
- Asian Journal of Psychiatry: SciencedirectDocument5 pagesAsian Journal of Psychiatry: SciencedirectRobiNo ratings yet
- Emotion Dysregulation and Negative Affect in Psychiatric SymptomsDocument18 pagesEmotion Dysregulation and Negative Affect in Psychiatric SymptomsRafael MartinsNo ratings yet
- 3721 FullDocument10 pages3721 FullLilianne Mbengani LaranjeiraNo ratings yet
- Angeles, Los Angeles, CaliforniaDocument1 pageAngeles, Los Angeles, CaliforniaJohn Loyd AlcasidNo ratings yet
- Proof 1Document11 pagesProof 1Erick Baltazar Ibarra FernandezNo ratings yet
- 10 1016@j Jaac 2016 09 023Document2 pages10 1016@j Jaac 2016 09 023Tlaloc GonzalezNo ratings yet
- Jurnal Schizophrenia PDFDocument10 pagesJurnal Schizophrenia PDFfathiyyahnurulNo ratings yet
- Zuckerman, M (1989) Personality in The Third Dimension A Psychobiological ApproachDocument28 pagesZuckerman, M (1989) Personality in The Third Dimension A Psychobiological ApproachMariana ArismendiNo ratings yet
- Correlatos Del Maltrato Físico en La Infancia en Mujeres Adultas Con Trastorno Distímico o Depresión MayorDocument8 pagesCorrelatos Del Maltrato Físico en La Infancia en Mujeres Adultas Con Trastorno Distímico o Depresión MayormagdaNo ratings yet
- Insight and Self-Stigma in Patients With Schizophrenia: Domagoj Vidović, Petrana Brečić, Maja Vilibić and Vlado JukićDocument6 pagesInsight and Self-Stigma in Patients With Schizophrenia: Domagoj Vidović, Petrana Brečić, Maja Vilibić and Vlado JukićAnđela MatićNo ratings yet
- Epilepsia - 2013 - Moschetta - Impulsivity and Seizure Frequency But Not Cognitive Deficits Impact Social Adjustment inDocument5 pagesEpilepsia - 2013 - Moschetta - Impulsivity and Seizure Frequency But Not Cognitive Deficits Impact Social Adjustment inilonaskorinNo ratings yet
- Teste Faux PasDocument5 pagesTeste Faux PasAdriano FerrazNo ratings yet
- Autistic Traits in The General Population: A Twin StudyDocument7 pagesAutistic Traits in The General Population: A Twin StudyVi KekaNo ratings yet
- Jamapsychiatry Bansal 2021 Oi 210069 1643689382.76996Document9 pagesJamapsychiatry Bansal 2021 Oi 210069 1643689382.76996hye soo kimNo ratings yet
- Prevalence, Persistence, and Sociodemographic Correlates of DSM-IV Disorders in The National Comorbidity Survey Replication Adolescent SupplementDocument18 pagesPrevalence, Persistence, and Sociodemographic Correlates of DSM-IV Disorders in The National Comorbidity Survey Replication Adolescent SupplementGaluh SabikhaNo ratings yet
- Illicit Psychoactive Substance Use, Heavy Use, Abuse, and Dependence in A US Population-Based Sample of Male TwinsDocument9 pagesIllicit Psychoactive Substance Use, Heavy Use, Abuse, and Dependence in A US Population-Based Sample of Male TwinsyuriNo ratings yet
- Emotional Intelligence and Personality in Major Depression: Trait Versus State EffectsDocument6 pagesEmotional Intelligence and Personality in Major Depression: Trait Versus State EffectsLaura AlfaroNo ratings yet
- Danckaerts2000 Article ANaturalHistoryOfHyperactivityDocument13 pagesDanckaerts2000 Article ANaturalHistoryOfHyperactivitymaksim6098No ratings yet
- Van Meter.2019.Bipolar Prodrome Symptom Scale - Abbreviated Screen For Patients: Description and ValidationDocument9 pagesVan Meter.2019.Bipolar Prodrome Symptom Scale - Abbreviated Screen For Patients: Description and ValidationGanellNo ratings yet
- Magallón-Neri 2018 Victimization AdolescentsDocument9 pagesMagallón-Neri 2018 Victimization AdolescentsuricomasNo ratings yet
- 2018 SAS Abstract Book C 0 PDFDocument80 pages2018 SAS Abstract Book C 0 PDFKhoa Le NguyenNo ratings yet
- Članak ShizofrenijaDocument6 pagesČlanak ShizofrenijaIvanNo ratings yet
- Prev Ans Depr CanverDocument6 pagesPrev Ans Depr CanverÉrico AugustoNo ratings yet
- Symptom Profiles of Autism Spectrum Disorder in Tuberous Sclerosis ComplexDocument14 pagesSymptom Profiles of Autism Spectrum Disorder in Tuberous Sclerosis ComplexWhyra Namikaze ComeyNo ratings yet
- Schizophrenia: SymptomsDocument8 pagesSchizophrenia: SymptomsVuong Linh GiangNo ratings yet
- CHORAggressionPsychopathology NOLAN JPsychRes2005Document7 pagesCHORAggressionPsychopathology NOLAN JPsychRes2005Leslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- RamelteonProductLabel 1218 PDFDocument18 pagesRamelteonProductLabel 1218 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- TriazolamProductLabel 1019 PDFDocument13 pagesTriazolamProductLabel 1019 PDFLeslie CitromeNo ratings yet
- DoxepinSleepProductLabel 0310 PDFDocument4 pagesDoxepinSleepProductLabel 0310 PDFLeslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
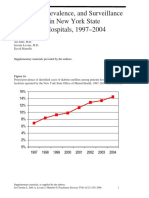
- Diabetes prevalence trends in NY mental hospitalsDocument8 pagesDiabetes prevalence trends in NY mental hospitalsLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- Catechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsDocument3 pagesCatechol-O-methyltransferase and Monoamine Oxidase-A Polymorphisms and Treatment Response To Typical and Atypical NeurolepticsLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster For Distribution CITROME CINP2006Leslie CitromeNo ratings yet
- Ziprasidone efficacy against hostility in schizophreniaDocument1 pageZiprasidone efficacy against hostility in schizophreniaLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- Incidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Document5 pagesIncidence and Prevalence of Diabetes in NY Psychiatric Hospitals 1997-2004Leslie CitromeNo ratings yet
- NR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaDocument1 pageNR330 Efficacy of Ziprasidone Against Hostility in SchizophreniaLeslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- ReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Document1 pageReducingInpatientAggressionPayingAttentionPaysOffPoster NOLAN APA2006Leslie CitromeNo ratings yet
- INTRODUCTION (Continued)Document1 pageINTRODUCTION (Continued)Leslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- QuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Document1 pageQuetiapineAntiaggressiveAgentCaseReport CITROME JCP2001Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- PDF Fcuk CTLG 2020 Split 01Document46 pagesPDF Fcuk CTLG 2020 Split 01Ted Andrew AbalosNo ratings yet
- Klee N Rite 50100Document24 pagesKlee N Rite 50100Nestor Marquez-DiazNo ratings yet
- Essential Oil Composition of Thymus Vulgaris L. and Their UsesDocument12 pagesEssential Oil Composition of Thymus Vulgaris L. and Their UsesAlejandro 20No ratings yet
- Adime Malnutrition and OncolgyDocument6 pagesAdime Malnutrition and Oncolgyapi-300587226100% (1)
- Measuring Blood Pressure AccuratelyDocument2 pagesMeasuring Blood Pressure AccuratelyxmantestNo ratings yet
- Connectwell Price List 2018 - W.E.F. 20.06.2018 PDFDocument110 pagesConnectwell Price List 2018 - W.E.F. 20.06.2018 PDFArun KumarNo ratings yet
- ETU 776 TripDocument1 pageETU 776 TripbhaskarinvuNo ratings yet
- CIE IGCSE BiologyDocument25 pagesCIE IGCSE Biologytgdzbspikio.comNo ratings yet
- Sage Yb October2015Document460 pagesSage Yb October2015olopNo ratings yet
- New Tunnel Boring MachineDocument7 pagesNew Tunnel Boring Machinealvaroaac4100% (1)
- CPC Sample Exam 1Document9 pagesCPC Sample Exam 1Renika_r80% (5)
- Sri LankaDocument2 pagesSri LankaADBGADNo ratings yet
- h04 High Sulphidation Epithermal Au Ag CuDocument6 pagesh04 High Sulphidation Epithermal Au Ag CuErenz Emerald AlexandriteNo ratings yet
- DH 201 To 300 Bedded Revised Draft PDFDocument158 pagesDH 201 To 300 Bedded Revised Draft PDFAmit Kumar MishraNo ratings yet
- Applications of Proton Exchange Membrane Fuel CellDocument20 pagesApplications of Proton Exchange Membrane Fuel CellRiri SasyNo ratings yet
- Dokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023Document23 pagesDokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023urexalg AlgériaNo ratings yet
- Under The Oak Tree Part 2Document94 pagesUnder The Oak Tree Part 2suakasenaNo ratings yet
- Fbioe 09 624021Document28 pagesFbioe 09 624021Davide Di ZioNo ratings yet
- Filter Integrity Test MachineDocument4 pagesFilter Integrity Test MachineAtul SharmaNo ratings yet
- Amal ResumeDocument2 pagesAmal ResumeMunaNo ratings yet
- Lecture Notes 12&13 Phylum ApicomplexaDocument20 pagesLecture Notes 12&13 Phylum ApicomplexaAmirr4uddinNo ratings yet
- Surgical Handpiece Maintenance PosterDocument2 pagesSurgical Handpiece Maintenance PosterHayes MaineNo ratings yet
- Parts of The CellDocument3 pagesParts of The Cellapi-308745623No ratings yet
- Diagnostic Test Science 5Document7 pagesDiagnostic Test Science 5Rex Russel SalemNo ratings yet
- Geotechnical Stability Guidelines PDFDocument24 pagesGeotechnical Stability Guidelines PDFAhmad Syafiq YudiansyahNo ratings yet
- PDFDocument478 pagesPDFPriyaranjan PradhanNo ratings yet
- EOA 2023 VISIOMER Portfolio Brochure en Digital RZ InteraktivDocument13 pagesEOA 2023 VISIOMER Portfolio Brochure en Digital RZ Interaktivichsan hakimNo ratings yet
- Pedest Tbox Toolbox - 4 Sidewalks and Walkways PDFDocument44 pagesPedest Tbox Toolbox - 4 Sidewalks and Walkways PDFbagibagifileNo ratings yet
- Phytochemical Analysis of Plant of Cissus QuadrangularisDocument7 pagesPhytochemical Analysis of Plant of Cissus QuadrangularisIJRASETPublicationsNo ratings yet
- GatesDocument188 pagesGatesMilos LIcko Bash RandjelovicNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)