You might also like
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
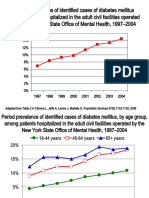
- DiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Document8 pagesDiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Leslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Leslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Leslie CitromeNo ratings yet
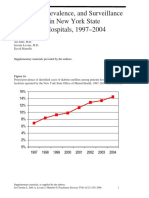
- DiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineDocument5 pagesDiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineLeslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Leslie CitromeNo ratings yet
- DivalproexDRtoERClinicalTrialAPA Poster CITROME APA2004Document1 pageDivalproexDRtoERClinicalTrialAPA Poster CITROME APA2004Leslie CitromeNo ratings yet
- Leslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDDocument1 pageLeslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDLeslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- MoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Document1 pageMoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Leslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Document1 pageZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Leslie CitromeNo ratings yet
- NewTreatmentsAgitationReview CITROME PsychQuarterly2004Document18 pagesNewTreatmentsAgitationReview CITROME PsychQuarterly2004Leslie CitromeNo ratings yet
- DosingSGAPosterWCBPHandout CITROME 2005Document4 pagesDosingSGAPosterWCBPHandout CITROME 2005Leslie CitromeNo ratings yet
- Mood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Document1 pageMood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Leslie CitromeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Stages of The Meth AddicitonDocument6 pagesThe Stages of The Meth AddicitonDegee O. Gonzales50% (2)
- Parent NewsletterDocument4 pagesParent Newsletterapi-301094873No ratings yet
- Developmental DisordersDocument58 pagesDevelopmental DisordersEsraRamos67% (3)
- Suneeta Monga, Diane Benoit - Assessing and Treating Anxiety Disorders in Young Children - The Taming Sneaky Fears Program-Springer International Publishing (2018)Document228 pagesSuneeta Monga, Diane Benoit - Assessing and Treating Anxiety Disorders in Young Children - The Taming Sneaky Fears Program-Springer International Publishing (2018)OlharapoNo ratings yet
- Internet AddictionDocument23 pagesInternet AddictionAdam Bullock100% (1)
- OCD and Related Disorders 1Document67 pagesOCD and Related Disorders 1Catherine Faith100% (1)
- Case Report: SymptomsDocument4 pagesCase Report: Symptomsapi-339983807No ratings yet
- Review: Deliberate Self-Harm and Suicide in AdolescentsDocument8 pagesReview: Deliberate Self-Harm and Suicide in AdolescentsIvy AntonioNo ratings yet
- Abnormal PsychologyDocument8 pagesAbnormal PsychologyAyanHamidNo ratings yet
- A Longitudinal Investigation of Mortality in Anorexia Nervosa and Bulimia NervosaDocument9 pagesA Longitudinal Investigation of Mortality in Anorexia Nervosa and Bulimia NervosaCarla MesquitaNo ratings yet
- Mental Illnesses in Children and Youth: Learn AboutDocument4 pagesMental Illnesses in Children and Youth: Learn AboutStefan BasilNo ratings yet
- Discuss Issues Relating To The Diagnosis and Classification of Schizophrenia. Essay For Unit 4 A Level Psychology AQA A. Typical Essay They Love To Ask Questions On.Document3 pagesDiscuss Issues Relating To The Diagnosis and Classification of Schizophrenia. Essay For Unit 4 A Level Psychology AQA A. Typical Essay They Love To Ask Questions On.moriya1012375% (4)
- Nursing Care Plan: Subjective: Nabalaka Ko Short Term: Independent: Goal Met Short TermDocument3 pagesNursing Care Plan: Subjective: Nabalaka Ko Short Term: Independent: Goal Met Short Termgeng gengNo ratings yet
- EmotionaryDocument1 pageEmotionaryMarceCoelloNo ratings yet
- Depersonalization Syndrome and HomeopathyDocument4 pagesDepersonalization Syndrome and HomeopathyAnonymous dpxYTENo ratings yet
- Multiple Choice Questions Multiple Choice QuestionsDocument19 pagesMultiple Choice Questions Multiple Choice QuestionsKay VinesNo ratings yet
- Draft Media ReleaseDocument4 pagesDraft Media Releaseapi-357857040No ratings yet
- Understanding The Vocational Impact of Mental Health Disorders.Document65 pagesUnderstanding The Vocational Impact of Mental Health Disorders.John F. LeporeNo ratings yet
- Mental Health Case StudyDocument11 pagesMental Health Case Studyapi-607361848No ratings yet
- Prader Willi SyndromeDocument19 pagesPrader Willi Syndromeluzmor13100% (1)
- Hyperlexia EssayDocument11 pagesHyperlexia Essayapi-286086829100% (1)
- Command Hallucinations, Compliance, and Risk Assessment: Keith Hersh, Ma, and Randy Borum, PsydDocument7 pagesCommand Hallucinations, Compliance, and Risk Assessment: Keith Hersh, Ma, and Randy Borum, PsydMiera ElmudhafieNo ratings yet
- ADHD and DepressionDocument8 pagesADHD and DepressionVicki B VeeNo ratings yet
- Mood DisordersDocument41 pagesMood Disordersdrali.kk4No ratings yet
- Informative Speech Outline (Asasi Tesl Uitm - LNS Assignment)Document5 pagesInformative Speech Outline (Asasi Tesl Uitm - LNS Assignment)Alya ShukNo ratings yet
- Suicide Risk Assessment - Pre-ReadDocument5 pagesSuicide Risk Assessment - Pre-ReadSaman HamidNo ratings yet
- Portfolio Output No. 13: Research On Anxiety Disorder/DepressionDocument7 pagesPortfolio Output No. 13: Research On Anxiety Disorder/DepressionAnnikah Trizya FACTONo ratings yet
- Personality Disorders PDFDocument19 pagesPersonality Disorders PDFrurban manipurNo ratings yet
- Obsessive Compulsive DisorderDocument12 pagesObsessive Compulsive DisorderMr. Psycho Sam100% (1)
- Abuse and ViolenceDocument152 pagesAbuse and ViolencePritam DugarNo ratings yet