You might also like
- Miller Anesthesia 7th Ed Chapter 34 Preop EvaluationDocument66 pagesMiller Anesthesia 7th Ed Chapter 34 Preop Evaluationjbahalkeh100% (1)
- Sample: Georgia Department of Public HealthDocument1 pageSample: Georgia Department of Public HealthWSB-TV Assignment DeskNo ratings yet
- SupplementStack PDFDocument19 pagesSupplementStack PDFbungureanu_6100% (1)
- Family Centered CareDocument7 pagesFamily Centered CareSirisha ChelvaNo ratings yet
- Book Preparing For Weight Loss Surgery Workbook PDFDocument140 pagesBook Preparing For Weight Loss Surgery Workbook PDFArran KennedyNo ratings yet
- Understanding Neurology - A Problem-Orientated Approach PDFDocument241 pagesUnderstanding Neurology - A Problem-Orientated Approach PDFAshabul AnharNo ratings yet
- NCP-Deficient Fluid VolumeDocument1 pageNCP-Deficient Fluid Volumejanmichael8No ratings yet
- Shatavari - Benefits, Precautions and DosageDocument13 pagesShatavari - Benefits, Precautions and Dosagenvenkatesh485No ratings yet
- Preoperative Assessment of Geriatric Patients Risks and Functional StatusDocument13 pagesPreoperative Assessment of Geriatric Patients Risks and Functional StatusruthchristinawibowoNo ratings yet
- Dien Bali Meeting 11Document5 pagesDien Bali Meeting 11Dien NingsihbaliNo ratings yet
- Diabetes Type 2 BasicsDocument44 pagesDiabetes Type 2 BasicsMasunji EmanuelNo ratings yet
- Jaffe Anesthesiologist Manual of Surgical ProcDocument50 pagesJaffe Anesthesiologist Manual of Surgical ProcHidayati IdaNo ratings yet
- The Family Doctor - Prof. Henry S Taylor, M.D., 1860Document324 pagesThe Family Doctor - Prof. Henry S Taylor, M.D., 1860IreneRainsNo ratings yet
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2No ratings yet
- Preoperative Patient Assessment and Management: Roxanne Jeen L. FornollesDocument61 pagesPreoperative Patient Assessment and Management: Roxanne Jeen L. FornollesRyan FornollesNo ratings yet
- 2014 Perioperative Slide SetDocument50 pages2014 Perioperative Slide SetAnonymous PcYFgC0YkNo ratings yet
- Preoperative Management of Patients Undergoing AnaesthesiaDocument24 pagesPreoperative Management of Patients Undergoing AnaesthesiaGx NavinNo ratings yet
- ECardDocument2 pagesECardsivaNo ratings yet
- MayoclinprocDocument12 pagesMayoclinprocpriyaNo ratings yet
- Preanesthesia IntroductionDocument38 pagesPreanesthesia IntroductionJovian LutfiNo ratings yet
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
- With Answers No RationaleDocument41 pagesWith Answers No RationaleronnaxNo ratings yet
- Pre Anesthetic EvaluationDocument67 pagesPre Anesthetic EvaluationdrvithalkNo ratings yet
- Tutorials in Surgery For 4th Medical StudentsDocument180 pagesTutorials in Surgery For 4th Medical StudentsAnonymous jSTkQVC27bNo ratings yet
- Anesthesia Pre Operative EvaluationDocument27 pagesAnesthesia Pre Operative EvaluationHassan.shehri100% (2)
- Stratification in The Older Adult For Operative RiskDocument24 pagesStratification in The Older Adult For Operative RiskshodhgangaNo ratings yet
- Rapid Geriatric Assessment of Hip FractureDocument14 pagesRapid Geriatric Assessment of Hip FractureJuliana Moreno LadinoNo ratings yet
- Perioperative Management of The Geriatric PatientDocument19 pagesPerioperative Management of The Geriatric PatientJunita Ratna SariNo ratings yet
- EndocrinoDocument15 pagesEndocrinoMichelle ElizaldeNo ratings yet
- Starr - Perioperative Assessment of and Care For The Elderly and Frail - Hospital Medicine Clinics - 5 - 2Document18 pagesStarr - Perioperative Assessment of and Care For The Elderly and Frail - Hospital Medicine Clinics - 5 - 2Yoga Mulia PratamaNo ratings yet
- 01. 麻醉前評估 - 陳坤堡Document58 pages01. 麻醉前評估 - 陳坤堡kenny631653No ratings yet
- Morgan 18 19Document83 pagesMorgan 18 19tri erdiansyahNo ratings yet
- Preoperative Evaluation Guide for Anesthesia and SurgeryDocument18 pagesPreoperative Evaluation Guide for Anesthesia and SurgeryanantosbiNo ratings yet
- Manejo Perioperativo Del Páciente Diabético en La Cirugía OrtopédicaDocument10 pagesManejo Perioperativo Del Páciente Diabético en La Cirugía OrtopédicaVicente David Treviño NavarroNo ratings yet
- Anesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFDocument11 pagesAnesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFtiaraleshaNo ratings yet
- J CPM 2019 02 010Document13 pagesJ CPM 2019 02 010Mohamed GoudaNo ratings yet
- Surgery and Anesthesia in Frail Older PatientsDocument68 pagesSurgery and Anesthesia in Frail Older PatientsWidiana SentotNo ratings yet
- What's New in Perioperative Cardiac TestingDocument17 pagesWhat's New in Perioperative Cardiac TestingCamilo HernándezNo ratings yet
- Evaluacion Pulmonar PreoperatoriaDocument15 pagesEvaluacion Pulmonar Preoperatorialuis castillejosNo ratings yet
- Perioperative Understandingofgeriatric Patients: Paris Payton,, Jeffrey E. ShookDocument10 pagesPerioperative Understandingofgeriatric Patients: Paris Payton,, Jeffrey E. Shookfabian arassiNo ratings yet
- Review Articles: Medical ProgressDocument10 pagesReview Articles: Medical ProgressMiko AkmarozaNo ratings yet
- Management of Common PostoperativeComplicationsDocument15 pagesManagement of Common PostoperativeComplicationsjamalNo ratings yet
- Anaesthesia For Major Urological SurgeryDocument23 pagesAnaesthesia For Major Urological SurgeryDianita P Ñáñez VaronaNo ratings yet
- Medical Evaluation of Surgical Patient 2015049Document39 pagesMedical Evaluation of Surgical Patient 2015049Kanneaufii KaramelNo ratings yet
- Preoperative Cardiac Risk AssessmentDocument16 pagesPreoperative Cardiac Risk Assessmentkrysmelis MateoNo ratings yet
- REVIEWER3Document33 pagesREVIEWER3Maye ArugayNo ratings yet
- Or AssignmentDocument3 pagesOr AssignmentMelissa Joy DollagaNo ratings yet
- J American Geriatrics Society - 2023 - Fountotos - Multicomponent Intervention For Frail and Pre Frail Older Adults WithDocument10 pagesJ American Geriatrics Society - 2023 - Fountotos - Multicomponent Intervention For Frail and Pre Frail Older Adults WithsilviaNo ratings yet
- Perioperative Management of Cardiac Patient For Noncardiac SurgeryDocument50 pagesPerioperative Management of Cardiac Patient For Noncardiac SurgeryPratistha SatyanegaraNo ratings yet
- Practice Advisory For Preanesthesia Evaluation. An Updated Report by The American Society of Anesthesiologists Task Force On PreanesthesiaDocument12 pagesPractice Advisory For Preanesthesia Evaluation. An Updated Report by The American Society of Anesthesiologists Task Force On PreanesthesiaMadalina TalpauNo ratings yet
- Terapia Dirigida Por Metas en Cirugía Cardíaca Lobdell2020Document10 pagesTerapia Dirigida Por Metas en Cirugía Cardíaca Lobdell2020Juan Guillermo BuitragoNo ratings yet
- Preoperative Assessment of The Older Patient: C.L. Pang, M. Gooneratne and J.S.L. PartridgeDocument7 pagesPreoperative Assessment of The Older Patient: C.L. Pang, M. Gooneratne and J.S.L. Partridgealejandro montesNo ratings yet
- Preanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFDocument86 pagesPreanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFCharlie Bellow100% (1)
- Enhanced Recovery AfterDocument14 pagesEnhanced Recovery Afterpiceng ismailNo ratings yet
- AGA Sirosis PreopDocument12 pagesAGA Sirosis PreopAlvy SyukrieNo ratings yet
- Surgery JournalDocument42 pagesSurgery JournalRose Ann RaquizaNo ratings yet
- Optimizing The Perioperative Nursing Role For The Older Adult Surgical PatientDocument5 pagesOptimizing The Perioperative Nursing Role For The Older Adult Surgical PatientLisha Marie GonzagaNo ratings yet
- Intro To Postop ComplicationsDocument11 pagesIntro To Postop ComplicationsRobert UntaruNo ratings yet
- Clin Diabetes 2001 Plodkowski 92 5Document4 pagesClin Diabetes 2001 Plodkowski 92 5Mahmoud SelimNo ratings yet
- Postoperative Care for Patients with Cardiovascular and Renal IssuesDocument6 pagesPostoperative Care for Patients with Cardiovascular and Renal IssuesAziil LiizaNo ratings yet
- Preoperative Cardiac Stress Testing A Thing of THDocument2 pagesPreoperative Cardiac Stress Testing A Thing of THDaiane GonçalvesNo ratings yet
- High Lactate Levels Are Predictors of Major Complications After Cardiac SurgeryDocument6 pagesHigh Lactate Levels Are Predictors of Major Complications After Cardiac SurgeryMuhammad RizqiNo ratings yet
- Preanesthesia IntroductionDocument38 pagesPreanesthesia IntroductionFendy WellenNo ratings yet
- Surgery Elderly 4Document5 pagesSurgery Elderly 4mx.pramirezNo ratings yet
- Articulo 1Document8 pagesArticulo 1Julio Cosme CastorenaNo ratings yet
- Pediatric Postoperative Cardiac CareDocument18 pagesPediatric Postoperative Cardiac CareChristian MartínezNo ratings yet
- Preoperative Evaluation For Non-Cardiac Surgery: AK GhoshDocument6 pagesPreoperative Evaluation For Non-Cardiac Surgery: AK GhoshAshvanee Kumar SharmaNo ratings yet
- Perioperative Management 26084 38335Document17 pagesPerioperative Management 26084 38335Olea CroitorNo ratings yet
- Anesthesiaforcolorectal Surgery: Gabriele Baldini,, William J. FawcettDocument31 pagesAnesthesiaforcolorectal Surgery: Gabriele Baldini,, William J. FawcettJEFFERSON MUÑOZNo ratings yet
- Non Cardiac OpDocument21 pagesNon Cardiac Opc4ri5No ratings yet
- Cad Fullguideline 510127Document8 pagesCad Fullguideline 510127Ana MariaNo ratings yet
- Preoperative Evaluation in The 21st CenturyDocument13 pagesPreoperative Evaluation in The 21st CenturyPaulHerrera0% (1)
- Biomarker-Based Preoperative Risk Stratification For Patients Undergoing Non-Cardiac Surgery - Yurttas Et Al 2020Document10 pagesBiomarker-Based Preoperative Risk Stratification For Patients Undergoing Non-Cardiac Surgery - Yurttas Et Al 2020santosfer1102No ratings yet
- Septic Arthritis: John J. Ross, MD, CMDocument19 pagesSeptic Arthritis: John J. Ross, MD, CMREY GARCIA DARIELA DEL VALLENo ratings yet
- Septic Arthritis: Basic InformationDocument5 pagesSeptic Arthritis: Basic InformationREY GARCIA DARIELA DEL VALLENo ratings yet
- Infectious Disease Trends Among Immunocompromised HostsDocument8 pagesInfectious Disease Trends Among Immunocompromised HostsREY GARCIA DARIELA DEL VALLENo ratings yet
- Male LUTS 2017 Pocket PDFDocument18 pagesMale LUTS 2017 Pocket PDFREY GARCIA DARIELA DEL VALLENo ratings yet
- Adverse Effects of Transfusion PDFDocument15 pagesAdverse Effects of Transfusion PDFREY GARCIA DARIELA DEL VALLENo ratings yet
- Worker Safety Perceptions in Low-Risk EnvironmentsDocument7 pagesWorker Safety Perceptions in Low-Risk Environmentstugas phiNo ratings yet
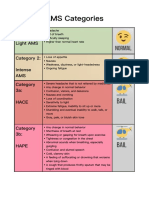
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Defining Preconception Exploring The ConceptDocument11 pagesDefining Preconception Exploring The Conceptrenno85No ratings yet
- Petkovski Dame Health RecordsDocument2 pagesPetkovski Dame Health RecordsMarijana PesevskiNo ratings yet
- 22 CR Protean NeurologicalDocument2 pages22 CR Protean NeurologicalCamii CvNo ratings yet
- Professional AdvancementDocument51 pagesProfessional AdvancementReshma AnilkumarNo ratings yet
- Report - Resource Based Conflicts and HR Violations in Protected AreasDocument83 pagesReport - Resource Based Conflicts and HR Violations in Protected AreasMagelah Peter GwayakaNo ratings yet
- Safety Data Sheet Sds/Msds Acrylamide For Electrophoresis MSDS CAS: 000079-06-1Document12 pagesSafety Data Sheet Sds/Msds Acrylamide For Electrophoresis MSDS CAS: 000079-06-1OladimejiNo ratings yet
- Trauma and Stressor-Related DisordersDocument58 pagesTrauma and Stressor-Related DisordersHamid Colangcag AmborNo ratings yet
- In vitro dissolution study of Metformin brandsDocument3 pagesIn vitro dissolution study of Metformin brandsrmahbub12No ratings yet
- (Cocos Nucifera) The Tree of Life: Coconut in Modern MedicineDocument6 pages(Cocos Nucifera) The Tree of Life: Coconut in Modern MedicineAdharsh ShankaranNo ratings yet
- Mabini National High School Midterm Exam ReviewDocument3 pagesMabini National High School Midterm Exam ReviewRoseann EnriquezNo ratings yet
- COSH Report - Sir KashmerDocument123 pagesCOSH Report - Sir Kashmerengr rangNo ratings yet
- B. Bruce Myers, MD PHD FACSDocument5 pagesB. Bruce Myers, MD PHD FACSallison8844No ratings yet
- English Task - Multiple Choices - 20200102Document8 pagesEnglish Task - Multiple Choices - 20200102bangtan's elite trashNo ratings yet
- Teks Diskusi PLPGDocument6 pagesTeks Diskusi PLPGKarlonius Bambang PurwantoNo ratings yet
- NBME Form 1 Step 2 ReviewDocument77 pagesNBME Form 1 Step 2 Reviewalex karevNo ratings yet