You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Features and ApplicationsDocument36 pagesFeatures and ApplicationsFWEFWEFWNo ratings yet
- Layout of Reverse CurveDocument7 pagesLayout of Reverse Curvem.ali. Sajjad100% (1)
- Seminar 4 & 5 - TelecomsDocument81 pagesSeminar 4 & 5 - TelecomsGible BubuNo ratings yet
- AuditingDocument47 pagesAuditingImran Alam ChowdhuryNo ratings yet
- How To Set WinDbg As A Default Windows Postmortem DebuggerDocument2 pagesHow To Set WinDbg As A Default Windows Postmortem DebuggeranilkumarjvjNo ratings yet
- Oxford Business English For Human ResourDocument1 pageOxford Business English For Human ResourАнастасия РезановаNo ratings yet
- MG PresentationDocument14 pagesMG PresentationsiddhNo ratings yet
- Characteristics of A Quality Asylum SystemDocument21 pagesCharacteristics of A Quality Asylum SystemAngel VermasNo ratings yet
- C8 Sanitary Design ChecklistDocument3 pagesC8 Sanitary Design ChecklistPoulami DeNo ratings yet
- Consolidated Financial Statements & Notes: Reliance Industries Limited Annual Report 2013-14Document7 pagesConsolidated Financial Statements & Notes: Reliance Industries Limited Annual Report 2013-14AdityaMahajanNo ratings yet
- Case: Pepe Jeans: Current Alternative 1 Alternative 2 Sales RevenueDocument1 pageCase: Pepe Jeans: Current Alternative 1 Alternative 2 Sales RevenueCristhian ValverdeNo ratings yet
- The Tiebout Model at Fifty, Ed. W.A. Fischel. Cambridge,: JEL ClassificationsDocument500 pagesThe Tiebout Model at Fifty, Ed. W.A. Fischel. Cambridge,: JEL ClassificationsJohnny Castillo SerapionNo ratings yet
- Torque Settings SV650SDocument17 pagesTorque Settings SV650SMrTwistNo ratings yet
- 2024년 수특+03강 유형별변형문제.hwpDocument59 pages2024년 수특+03강 유형별변형문제.hwpzhengyujin28No ratings yet
- (IBM) System Storage SAN Volume Controller Version 6.4.0Document350 pages(IBM) System Storage SAN Volume Controller Version 6.4.0hiehie272No ratings yet
- Iso Astm 51026-15Document9 pagesIso Astm 51026-15TertulianoPintoNo ratings yet
- Pilz PSS 3056 Series Manual PDFDocument49 pagesPilz PSS 3056 Series Manual PDFRobin CruzNo ratings yet
- Credit Card Market EntryDocument4 pagesCredit Card Market EntryaqaiserNo ratings yet
- Effective Date: May, 2004Document27 pagesEffective Date: May, 2004AlbertoNo ratings yet
- User Manual Reports FINGate PortalDocument103 pagesUser Manual Reports FINGate PortalAbhinav BharadwajNo ratings yet
- Oil PalmDocument2 pagesOil PalmPOLTAKSIHOMBINGNo ratings yet
- Kat - Ersce - EngDocument28 pagesKat - Ersce - EngCsaba VargaNo ratings yet
- IA Rubric Requirements - ChecklistDocument1 pageIA Rubric Requirements - ChecklistRITA CHANDRANNo ratings yet
- Wastage in A RestaurantDocument5 pagesWastage in A RestaurantLukeni AraujoNo ratings yet
- Application LetterDocument5 pagesApplication Lettersdguillermo928No ratings yet
- 999dice Bot Super Profit Alberto Gambler DogeDocument190 pages999dice Bot Super Profit Alberto Gambler DogeMI PattapangNo ratings yet
- Single-Zone Heating and Cooling Systems Daikin Aurora: High Capacity Models Available!Document6 pagesSingle-Zone Heating and Cooling Systems Daikin Aurora: High Capacity Models Available!Dhaval JoshiNo ratings yet
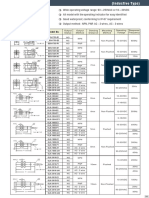
- Outline Dimension Model No .: Output Status Output Method Sensing Distance Mounting MethodDocument2 pagesOutline Dimension Model No .: Output Status Output Method Sensing Distance Mounting MethodAgus YohanesNo ratings yet
- Writing Business Messages ActivitiesDocument9 pagesWriting Business Messages Activitiesshumaila parveenNo ratings yet
- Modeling and Simulation of Hybrid Solar-Wind Energy System Using MPPT AlgorithmDocument13 pagesModeling and Simulation of Hybrid Solar-Wind Energy System Using MPPT Algorithmmohammed.abdullaNo ratings yet