You might also like
- BA JapanesePG PDFDocument7 pagesBA JapanesePG PDFIan IskandarNo ratings yet
- Design ParameterDocument13 pagesDesign ParameterkennysawegNo ratings yet
- Zero Carbon Building StandardsDocument32 pagesZero Carbon Building Standardsjoslinmtg100% (1)
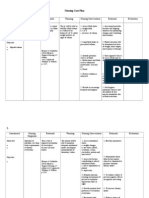
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- Service Manual: Autoclave Sterilising Sterilclave 18/24Document29 pagesService Manual: Autoclave Sterilising Sterilclave 18/24hüseyin vururNo ratings yet
- Blue ProtocolDocument11 pagesBlue Protocoloana florianaNo ratings yet
- Transportation EngineeringDocument312 pagesTransportation EngineeringCourtney Ward75% (4)
- Respiratory Distress Syndrome LapkasDocument49 pagesRespiratory Distress Syndrome LapkasThamarai SomuNo ratings yet
- Ryan Ronquillo ComplaintDocument39 pagesRyan Ronquillo ComplaintMichael_Lee_RobertsNo ratings yet
- Smart AntennasDocument40 pagesSmart AntennasMeeraNo ratings yet
- Neonatal Respiratory Distress Syndrome: Chest X-Ray or Lung Ultrasound? A Systematic ReviewDocument12 pagesNeonatal Respiratory Distress Syndrome: Chest X-Ray or Lung Ultrasound? A Systematic ReviewMonika JonesNo ratings yet
- Boursiani 2017Document5 pagesBoursiani 2017Carlos Urkieta MonetaNo ratings yet
- Clinical Characteristics, Diagnosis, and Management Outcome of SurfactantDocument7 pagesClinical Characteristics, Diagnosis, and Management Outcome of SurfactantakshayajainaNo ratings yet
- Tto Crup NatureDocument7 pagesTto Crup NatureCarolina Mora RuedaNo ratings yet
- Prediciendo SDR Usando Espectroscopía Del Residuo Gástrico - ClínicaDocument6 pagesPrediciendo SDR Usando Espectroscopía Del Residuo Gástrico - ClínicaRonald MoralesNo ratings yet
- ProdukteDocument6 pagesProdukteGaurav SharmaNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhaDocument6 pagesSeminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhadeniNo ratings yet
- Neonatal Respiratory Distress Syndrome: Chest X-Ray or Lung Ultrasound? A Systematic ReviewDocument13 pagesNeonatal Respiratory Distress Syndrome: Chest X-Ray or Lung Ultrasound? A Systematic ReviewMeiriyani LembangNo ratings yet
- Laryngeal Measurements and Diagnostic Tools For Diag-Nosis of Chronic Obstructive Pulmonary DiseaseDocument4 pagesLaryngeal Measurements and Diagnostic Tools For Diag-Nosis of Chronic Obstructive Pulmonary DiseaseBudi RiyantoNo ratings yet
- SDR Segun EdadDocument9 pagesSDR Segun EdadLuzbenia ChaparroNo ratings yet
- A Radiological Perspective of Assessing Neonatal Respiratory Distress SyndromeDocument6 pagesA Radiological Perspective of Assessing Neonatal Respiratory Distress Syndromeyoga zunandy pratamaNo ratings yet
- Sleep Disordered Breathing in Patients With Chronic Kidney Diseases How Far The ProblemDocument13 pagesSleep Disordered Breathing in Patients With Chronic Kidney Diseases How Far The ProblemJohn RonquilloNo ratings yet
- Ultrasonido Doppler Temprano AMSDocument7 pagesUltrasonido Doppler Temprano AMSKaren Marbelly OrozcoNo ratings yet
- Early Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaDocument9 pagesEarly Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaHerbert Baquerizo VargasNo ratings yet
- Patterns of Radiographic Findings in Pediatric Chest Radiographs in EnugustDocument5 pagesPatterns of Radiographic Findings in Pediatric Chest Radiographs in Enugustمحمد عبد القاهر السروريNo ratings yet
- BMM 2018 0348Document14 pagesBMM 2018 0348Harpreet SinghNo ratings yet
- Value of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaDocument5 pagesValue of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaHarlan SiMarmutNo ratings yet
- Prediction of Extubation Readiness Using Lung Ultrasound in Preterm InfantsDocument8 pagesPrediction of Extubation Readiness Using Lung Ultrasound in Preterm InfantsAlexandra NemesNo ratings yet
- Respiratory Distress SyndromeeDocument42 pagesRespiratory Distress SyndromeeRoman MamunNo ratings yet
- Dyke 2023 Ped Radiol PREFUL Lung MRI Ventilation NICUDocument9 pagesDyke 2023 Ped Radiol PREFUL Lung MRI Ventilation NICUJonathan DykeNo ratings yet
- Scintigraphic GastroesophagealDocument7 pagesScintigraphic GastroesophagealMarylin Acuña HernándezNo ratings yet
- AMJ-Volume 50-Issue 2 - Page 1489-1496Document8 pagesAMJ-Volume 50-Issue 2 - Page 1489-1496Pandu Putra Wijaya RestaNo ratings yet
- Effect of Hemodynamic Significant Patent Ductus Arteriosus On Tissue Oxygenation in Preterm Infants Using Near-Infrared SpectrosDocument7 pagesEffect of Hemodynamic Significant Patent Ductus Arteriosus On Tissue Oxygenation in Preterm Infants Using Near-Infrared SpectrosLissaberti AmaliahNo ratings yet
- Detection of Placenta Acreta in The First Trimester by 2d Transvaginal Ultrasound and Colour DopplerDocument14 pagesDetection of Placenta Acreta in The First Trimester by 2d Transvaginal Ultrasound and Colour DopplerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal ReadingDocument5 pagesJournal ReadingRoma WestNo ratings yet
- Saul Salamat RDSDocument6 pagesSaul Salamat RDShoneyailbhatti53No ratings yet
- JurnalDocument6 pagesJurnalIzzyNo ratings yet
- Ajukan 2Document12 pagesAjukan 2Rifky TaniyoNo ratings yet
- Clinical Predictors of Radiographic Abnormalities Among Infants With Bronchiolitis in A Paediatric Emergency DepartmentDocument5 pagesClinical Predictors of Radiographic Abnormalities Among Infants With Bronchiolitis in A Paediatric Emergency Departmentnavali rahmaNo ratings yet
- Diagnosis of Pneumonia in Children With Dehydrating DiarrhoeaDocument6 pagesDiagnosis of Pneumonia in Children With Dehydrating DiarrhoeaEmaa AmooraNo ratings yet
- CCRPM 2011 001 PDFDocument5 pagesCCRPM 2011 001 PDFAlexandria Firdaus Al-farisyNo ratings yet
- 699-Article Text-1085-1-10-20181101Document6 pages699-Article Text-1085-1-10-20181101Shahid HussainNo ratings yet
- Improving Risk Stratification of Rheumatoid Arthritis Patients For Intestinal Lung DiseasesDocument11 pagesImproving Risk Stratification of Rheumatoid Arthritis Patients For Intestinal Lung DiseasesdopiorototoNo ratings yet
- CPAP For Prevention CVE in OSADocument13 pagesCPAP For Prevention CVE in OSAenNo ratings yet
- En Aop06912Document9 pagesEn Aop06912Dian Putri NingsihNo ratings yet
- Jurnal RespiDocument5 pagesJurnal RespiReza MaulanaNo ratings yet
- Medi 101 E29940Document5 pagesMedi 101 E29940Bella FebriantiNo ratings yet
- Usg Pada TB PulmoDocument8 pagesUsg Pada TB Pulmoaradana wahyudaNo ratings yet
- Evaluation of Compliance With Standard Criteria For Postero-Anterior (Pa) Chest Radiographs in Parklane Hospital EnuguDocument37 pagesEvaluation of Compliance With Standard Criteria For Postero-Anterior (Pa) Chest Radiographs in Parklane Hospital EnuguLavinia VictorNo ratings yet
- Etiological Study of Respiratory Distress in Newborn: Original ResearchDocument5 pagesEtiological Study of Respiratory Distress in Newborn: Original ResearchNovia KurniantiNo ratings yet
- A88 Nirs PdaDocument9 pagesA88 Nirs PdaFahri OvalıNo ratings yet
- BIBOSO, Christine Marie BILLONES, Beverly Ann BSN4-CDocument30 pagesBIBOSO, Christine Marie BILLONES, Beverly Ann BSN4-CPrecious La-anan BibosoNo ratings yet
- Vap NicuDocument8 pagesVap NicuWiwit ClimberNo ratings yet
- Buonsenso Et Al-2018-Pediatric PulmonologyDocument9 pagesBuonsenso Et Al-2018-Pediatric Pulmonologywawa chenNo ratings yet
- Journal Pone 0000192Document5 pagesJournal Pone 0000192TriponiaNo ratings yet
- Jurnal Pubme 1 RdsDocument13 pagesJurnal Pubme 1 Rdsriri risna aNo ratings yet
- Clinical Profile, Etiology, and Management of Hydropneumothorax: An Indian ExperienceDocument5 pagesClinical Profile, Etiology, and Management of Hydropneumothorax: An Indian ExperienceSarah DaniswaraNo ratings yet
- Autogenic 1 PDFDocument5 pagesAutogenic 1 PDFpermanaNo ratings yet
- Nirs Preterm ScreeenDocument6 pagesNirs Preterm ScreeenLissaberti AmaliahNo ratings yet
- Analysis of Age-Related Prevalence and Risk Factors of Chronic Rhinosinusitis With AsthmaDocument7 pagesAnalysis of Age-Related Prevalence and Risk Factors of Chronic Rhinosinusitis With AsthmaAnnisa Dhiya UlhaqNo ratings yet
- A Belgian Survey On The Diagnosis of Asthma - COPD Overlap SyndromeDocument13 pagesA Belgian Survey On The Diagnosis of Asthma - COPD Overlap SyndromesyahrulNo ratings yet
- Chest Radiographic Manifestations of Scrub Typhus - PMCDocument9 pagesChest Radiographic Manifestations of Scrub Typhus - PMCSurachai PraimaiNo ratings yet
- Diagnostic Use of Lung Ultrasound Compared To Chest Radiograph For Suspected Pneumonia in A Resource-Limited SettingDocument5 pagesDiagnostic Use of Lung Ultrasound Compared To Chest Radiograph For Suspected Pneumonia in A Resource-Limited SettingGhaisani Nur ShabrinaNo ratings yet
- Usefulness of Tumor Marker CA-125 Serum Levels For The Follow-Up of Therapeutic Responses in Tuberculosis Patients With and Without SerositisDocument6 pagesUsefulness of Tumor Marker CA-125 Serum Levels For The Follow-Up of Therapeutic Responses in Tuberculosis Patients With and Without Serositishumayun kabirNo ratings yet
- Usg HMDDocument5 pagesUsg HMDBunga alaraafNo ratings yet
- Rodriguez G - Serum ACE Activity in Normal Children and in Those With SarcoidosisDocument5 pagesRodriguez G - Serum ACE Activity in Normal Children and in Those With SarcoidosisPhaimNo ratings yet
- (2009) Radiographic Improvement and Its Predictors in Patients With Pulmonary TuberculosisDocument6 pages(2009) Radiographic Improvement and Its Predictors in Patients With Pulmonary TuberculosisMohd RahimiNo ratings yet
- Discrete Variable RepresentationDocument4 pagesDiscrete Variable RepresentationJustin BrockNo ratings yet
- Tetrasteel 800 BrochureDocument4 pagesTetrasteel 800 BrochurejcrandleNo ratings yet
- Para Jumbles Test-1Document4 pagesPara Jumbles Test-1vennelaNo ratings yet
- Anatomy of A FireworkDocument4 pagesAnatomy of A FireworkMuthu KumarNo ratings yet
- The IMA Volumes in Mathematics and Its Applications: Avner Friedman Willard Miller, JRDocument172 pagesThe IMA Volumes in Mathematics and Its Applications: Avner Friedman Willard Miller, JRPedro PereyraNo ratings yet
- 7 140706224638 Phpapp01Document165 pages7 140706224638 Phpapp01Theodøros D' Spectrøøm0% (1)
- Abstract CV: Maharani Retna Duhita, M.SC.,PHD - Med.ScDocument39 pagesAbstract CV: Maharani Retna Duhita, M.SC.,PHD - Med.ScnanaNo ratings yet
- Ijesrt: International Journal of Engineering Sciences & Research TechnologyDocument11 pagesIjesrt: International Journal of Engineering Sciences & Research TechnologyAna MariaNo ratings yet
- Dr. BM RAO - Nitrosamine Impurities and NDSRIs UpdatesDocument5 pagesDr. BM RAO - Nitrosamine Impurities and NDSRIs UpdatesVinay PatelNo ratings yet
- Bitting Your Horse BlueprintDocument17 pagesBitting Your Horse BlueprintPaola TorresNo ratings yet
- Rohini 24928786475Document12 pagesRohini 24928786475aswinvirat84No ratings yet
- MCqs & Q Ans For Class 9Document61 pagesMCqs & Q Ans For Class 9Shahbaz Siddikie100% (1)
- Layer 3 48-Port 10G SFP+ + 2-Port 40G QSFP+ + 4-Port 100G QSFP28 Managed SwitchDocument10 pagesLayer 3 48-Port 10G SFP+ + 2-Port 40G QSFP+ + 4-Port 100G QSFP28 Managed Switchbader eddine khezamiNo ratings yet
- The 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsDocument51 pagesThe 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsAmAnDeepSingh100% (1)
- Worksheet of EDC - 2018Document2 pagesWorksheet of EDC - 2018pranavmurthyNo ratings yet
- Mobile: +91 9245560892 Objective: N.RaghunathanDocument3 pagesMobile: +91 9245560892 Objective: N.RaghunathanRagunathan NarayananNo ratings yet
- Indore BrtsDocument22 pagesIndore BrtsRaj PatelNo ratings yet
- Types of ProductionDocument2 pagesTypes of ProductionromwamaNo ratings yet
- Study On Solar Irrigation System in BangladeshDocument61 pagesStudy On Solar Irrigation System in Bangladeshavocadocolor100% (2)
- TEST SHEET139: 2021-2022: TERM: 1: Section B: Text AnalysisDocument2 pagesTEST SHEET139: 2021-2022: TERM: 1: Section B: Text AnalysisLavanya SharmaNo ratings yet
- Harga Satuan Precast 2017Document2 pagesHarga Satuan Precast 2017GenTigaBrotherhood BantenNo ratings yet
- OriginalDocument19 pagesOriginalGoma SelvaraniNo ratings yet