You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- CE1001 Basic CivilDocument3 pagesCE1001 Basic CivilMayank AgarwalNo ratings yet
- Ultra 1Document27 pagesUltra 1VishnuNo ratings yet
- IVP Practical ManualDocument63 pagesIVP Practical ManualPunam SindhuNo ratings yet
- IrprodguideDocument82 pagesIrprodguideNalin Lochan GuptaNo ratings yet
- Weekly Industrial Training Report Mohd Izzat - Week 1Document3 pagesWeekly Industrial Training Report Mohd Izzat - Week 1Izzat FakhriNo ratings yet
- RXV2700Document173 pagesRXV2700Евгений ЗахаровNo ratings yet
- Ibisworld Industry: Global Computer Hardware ManufacturingDocument49 pagesIbisworld Industry: Global Computer Hardware ManufacturingYuk Ming WongNo ratings yet
- BSIL Questionnaire For Gin and Press - P & M (03!11!17)Document1 pageBSIL Questionnaire For Gin and Press - P & M (03!11!17)michael odiemboNo ratings yet
- Anemometro Sper Scientific PDFDocument1 pageAnemometro Sper Scientific PDFalez91No ratings yet
- G. Paul, Et Al., A Simplified Predictive Model For Micellar-Polymer Flooding PDFDocument20 pagesG. Paul, Et Al., A Simplified Predictive Model For Micellar-Polymer Flooding PDFRaemora Zaith IthinNo ratings yet
- Binocular Hands and Head Tracking Using Projective Joint Probabilistic Data Association FilterDocument50 pagesBinocular Hands and Head Tracking Using Projective Joint Probabilistic Data Association FilterMiyabi MayoNo ratings yet
- Using The DHT11 Sensor With Raspberry Pi To Measure Temperature and HumidityDocument3 pagesUsing The DHT11 Sensor With Raspberry Pi To Measure Temperature and HumidityVimalNo ratings yet
- 141 - CATALOG Plasma Esab 2018 TalasDocument23 pages141 - CATALOG Plasma Esab 2018 TalasHector BarriosNo ratings yet
- Indian Railways Vision For Future: Vol Iii Development of Mathura JN As World Class StationDocument8 pagesIndian Railways Vision For Future: Vol Iii Development of Mathura JN As World Class Stationvijendra SutharNo ratings yet
- Transformer Protection Calculations PDFDocument44 pagesTransformer Protection Calculations PDFngocanhvyNo ratings yet
- ATO System: Civil Aviation Authority of The PhilippinesDocument5 pagesATO System: Civil Aviation Authority of The Philippineskimberley dela cruzNo ratings yet
- HYSYSDocument390 pagesHYSYSEfosaUwaifoNo ratings yet
- Manual 99 LDDocument20 pagesManual 99 LDCristianNo ratings yet
- Programming User RPLIn PCDocument26 pagesProgramming User RPLIn PCselm27No ratings yet
- MODULE 5 Alternativebuildingmaterials PDFDocument28 pagesMODULE 5 Alternativebuildingmaterials PDFPreethi SrinivasNo ratings yet
- Ishikawa Diagram: For PowerpointDocument3 pagesIshikawa Diagram: For PowerpointSudhagarNo ratings yet
- Chrysler GroupDocument12 pagesChrysler Groupfrancisca19No ratings yet
- Sig 550 and 551 Assault Rifle User ManualDocument56 pagesSig 550 and 551 Assault Rifle User ManualGasMaskBob100% (1)
- Hi Survey User Manual en 20230428Document314 pagesHi Survey User Manual en 20230428tinaNo ratings yet
- WP - Wholesale - BM ItemsDocument2 pagesWP - Wholesale - BM ItemsRenato OrosaNo ratings yet
- My Resume Updated ...Document4 pagesMy Resume Updated ...ClydeGutierrezNo ratings yet
- Smartform QuestionDocument14 pagesSmartform QuestionrohanNo ratings yet
- Teste Pe TestDocument40 pagesTeste Pe TestINformai hkdskdhNo ratings yet
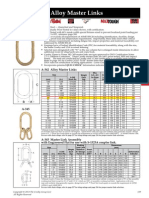
- Crosby Alloy MasterlinkDocument1 pageCrosby Alloy MasterlinkjakashNo ratings yet
- OrnithopterDocument12 pagesOrnithopterDhirajNo ratings yet