You might also like
- Decree 4725 de 2005Document3 pagesDecree 4725 de 2005api-594576766No ratings yet
- 10 1016@j JHT 2017 02 001 PDFDocument10 pages10 1016@j JHT 2017 02 001 PDFGusti Ayu KrisnayantiNo ratings yet
- Jaccoa 08 00330Document5 pagesJaccoa 08 00330Teshome AssefaNo ratings yet
- Postdural Puncture Headache: Kyung-Hwa KwakDocument8 pagesPostdural Puncture Headache: Kyung-Hwa KwakRakha FahrezaNo ratings yet
- Deambulacion Vs Reposo en CPPDocument10 pagesDeambulacion Vs Reposo en CPPNoé Alejandro SánchezNo ratings yet
- Postdural Puncture Headache and Epidural Blood Patch Use in Elderly PatientsDocument5 pagesPostdural Puncture Headache and Epidural Blood Patch Use in Elderly PatientsJunwei XingNo ratings yet
- PDPH MeruDocument6 pagesPDPH MeruTeshome AssefaNo ratings yet
- Management Practices For Postdural Puncture Headache in Obstetrics: A Prospective, International, Cohort StudyDocument11 pagesManagement Practices For Postdural Puncture Headache in Obstetrics: A Prospective, International, Cohort StudyAlexisNo ratings yet
- Post Dural Puncture Headache - UpToDateDocument17 pagesPost Dural Puncture Headache - UpToDateBarbarita Alvarado CamposNo ratings yet
- Stroke - Severity - Modified - The - Effect - of - Chronic.66 TromboliziraniDocument5 pagesStroke - Severity - Modified - The - Effect - of - Chronic.66 TromboliziraniM StojanovskaNo ratings yet
- Panic Disorder in Patients Presenting To The Emergency Department With Chest Pain: Prevalence and Presenting SymptomsDocument7 pagesPanic Disorder in Patients Presenting To The Emergency Department With Chest Pain: Prevalence and Presenting SymptomsNasriNo ratings yet
- International Journal of Surgery Case Reports: Mekuanint Asmare, Liyew Ewnetu, Kumlachew GetaDocument3 pagesInternational Journal of Surgery Case Reports: Mekuanint Asmare, Liyew Ewnetu, Kumlachew GetanukeNo ratings yet
- HypertensiDocument7 pagesHypertensizazaNo ratings yet
- Jurnal UtamaDocument8 pagesJurnal UtamaUhti JahrotunisaNo ratings yet
- Neshige 2015Document5 pagesNeshige 2015belleswanNo ratings yet
- A Study On Assessment of Frequency, Intensity, Disability and Severity Associated With Primary HeadachesDocument7 pagesA Study On Assessment of Frequency, Intensity, Disability and Severity Associated With Primary HeadachesDhEg LieShh WowhNo ratings yet
- Pain Agitation DeliriumDocument10 pagesPain Agitation DeliriumMelati HasnailNo ratings yet
- 22 Ajner 7 1 2017Document8 pages22 Ajner 7 1 2017Aqnha AulyaNo ratings yet
- BallDocument8 pagesBallAllan Alejandro SevillaNo ratings yet
- Thailand Anest,+02-Raviwan-FinalDocument8 pagesThailand Anest,+02-Raviwan-FinalAldaherlen BangunNo ratings yet
- The Effectiveness of Early Position Change Postcardiac Catheterization On Patient's Outcomes A Randomized Controlled TrialDocument9 pagesThe Effectiveness of Early Position Change Postcardiac Catheterization On Patient's Outcomes A Randomized Controlled TrialAdelia putriNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Medi 97 E10919Document4 pagesMedi 97 E10919oktaviaNo ratings yet
- 21 Iajps21072017Document4 pages21 Iajps21072017Baru Chandrasekhar RaoNo ratings yet
- StudyDocument23 pagesStudyJose Paul RaderNo ratings yet
- Cefalea PospuncionDocument31 pagesCefalea Pospuncionmanolo.mendozavNo ratings yet
- 26 PDFDocument5 pages26 PDFBaru Chandrasekhar RaoNo ratings yet
- A Comprehensive Update On The Treatment and Management of Postdural Puncture HeadacheDocument9 pagesA Comprehensive Update On The Treatment and Management of Postdural Puncture HeadacheFirjatullahNo ratings yet
- Korea Video ProgramDocument12 pagesKorea Video Programmaya permata sariNo ratings yet
- Comparision Between Provisional Diagnosis Made in Emergency Department VS Final Discharge Diagnosis at Ramkrishna Care Hospital, Raipur C.GDocument14 pagesComparision Between Provisional Diagnosis Made in Emergency Department VS Final Discharge Diagnosis at Ramkrishna Care Hospital, Raipur C.GIJAR JOURNALNo ratings yet
- Treatment Options For Patellar Tendinopathy: A Systematic ReviewDocument12 pagesTreatment Options For Patellar Tendinopathy: A Systematic ReviewEstefa Roldan RoldanNo ratings yet
- Effectiveness of Chinese Hand Massage On Anxiety Among Patients Awaitng Coronary AngiographyDocument8 pagesEffectiveness of Chinese Hand Massage On Anxiety Among Patients Awaitng Coronary AngiographyLia AgustinNo ratings yet
- Research Article Published in Plose One - Manish Chandra PrabhakarDocument6 pagesResearch Article Published in Plose One - Manish Chandra PrabhakarManish Chandra Prabhakar100% (1)
- Treatment Options For Patellar Tendinopathy A Systematic ReviewDocument12 pagesTreatment Options For Patellar Tendinopathy A Systematic ReviewRonny Araya AbarcaNo ratings yet
- Postdural Puncture Headache A Headache ARTICULO 1Document8 pagesPostdural Puncture Headache A Headache ARTICULO 1alejandro rodriguezNo ratings yet
- HHS Public AccessDocument14 pagesHHS Public AccessPepe OcaNo ratings yet
- Swallowing Rehabilitation Following Spinal Injury A Case SeriesDocument12 pagesSwallowing Rehabilitation Following Spinal Injury A Case SeriesniekoNo ratings yet
- Quotes On ESIsDocument2 pagesQuotes On ESIsArt Levine, Mental Health Inc.No ratings yet
- Study To Determine The Role of Platelet Rich Plasma Injection in Treatment of Frozen Shoulder in Terms of Improvement in PainDocument5 pagesStudy To Determine The Role of Platelet Rich Plasma Injection in Treatment of Frozen Shoulder in Terms of Improvement in PainEditor IJETBSNo ratings yet
- Precedex Delirium Spine - AA2023Document9 pagesPrecedex Delirium Spine - AA2023Ahida VelazquezNo ratings yet
- Plan of Thesis VishalDocument24 pagesPlan of Thesis Vishalvishaljha86No ratings yet
- DrugDocument7 pagesDrugIhdina Hanifa Hasanal IbrahimNo ratings yet
- Rooij Et Al-2016-Arthritis Care & ResearchDocument12 pagesRooij Et Al-2016-Arthritis Care & ResearchJennifer JaneNo ratings yet
- The Outcomes of Serial Cerebrospinal Fluid Removal in Elderly Patients With Idiopathic Normal Pressure HydrocephalusDocument7 pagesThe Outcomes of Serial Cerebrospinal Fluid Removal in Elderly Patients With Idiopathic Normal Pressure Hydrocephalusmutia nur rahmiNo ratings yet
- Investigating The Impact of Foot Reflexology On SeDocument6 pagesInvestigating The Impact of Foot Reflexology On Segitha noviaNo ratings yet
- IJTPR, Vol 13, Issue 10, Article 8Document4 pagesIJTPR, Vol 13, Issue 10, Article 8Jaldeep PatelNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofnaufal12345No ratings yet
- Giovannetti (2019) - Cognition and Cerebral Infarction in Older Adults After Surgical Aortic Valve ReplacementDocument8 pagesGiovannetti (2019) - Cognition and Cerebral Infarction in Older Adults After Surgical Aortic Valve ReplacementVanessaNo ratings yet
- 2020 Invasive Electrical Neuromodulation For The Treatment of Painful Diabetic Neuropathy Systematic Review and Meta-AnalysisDocument9 pages2020 Invasive Electrical Neuromodulation For The Treatment of Painful Diabetic Neuropathy Systematic Review and Meta-AnalysisSafitri MuhlisaNo ratings yet
- Pulsed Radiofrequency ofDocument8 pagesPulsed Radiofrequency ofDiego Pinto PatroniNo ratings yet
- Assessment of The Effect of Epidural Steroid Injection in Patient Having Lumbar RadiculopathyDocument5 pagesAssessment of The Effect of Epidural Steroid Injection in Patient Having Lumbar RadiculopathyIJAR JOURNALNo ratings yet
- Acute LBP ScreenDocument6 pagesAcute LBP ScreenIsnaenyEraKartikaNo ratings yet
- Murottal Al-Qur'An Stimulation For Reducing Anxiety Level On Acute Coronary Syndrome Patient: A Practice Based On EvidenceDocument9 pagesMurottal Al-Qur'An Stimulation For Reducing Anxiety Level On Acute Coronary Syndrome Patient: A Practice Based On EvidenceDesi Ratna SariNo ratings yet
- Chen 2017Document7 pagesChen 2017Miranti Dea DoraNo ratings yet
- Extubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryDocument9 pagesExtubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryEdison LucioNo ratings yet
- Efects of Splinting in EpicondylitisDocument8 pagesEfects of Splinting in EpicondylitisMaria Jesus GonzalezNo ratings yet
- Post Swallowing DysfunctionDocument7 pagesPost Swallowing DysfunctionfitrianisyaNo ratings yet
- Patient Safety During Sedation by Anesthesia ProfeDocument8 pagesPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoNo ratings yet
- Content ServerDocument13 pagesContent ServerTisna WennyNo ratings yet
- Assessment of The Effects of Dysphagia Therapy in Patients in The Early Post-Stroke Period: A Randomised Controlled TrialDocument7 pagesAssessment of The Effects of Dysphagia Therapy in Patients in The Early Post-Stroke Period: A Randomised Controlled TrialAlba Fernández GonzálezNo ratings yet
- Kidney Transplant Management: A Guide to Evaluation and ComorbiditiesFrom EverandKidney Transplant Management: A Guide to Evaluation and ComorbiditiesNo ratings yet
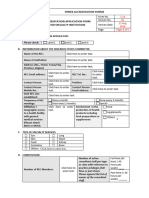
- PHREB Form No. 1.1a Application For Accreditationof Specialty ClinicsDocument5 pagesPHREB Form No. 1.1a Application For Accreditationof Specialty ClinicsDawn CasuncadNo ratings yet
- Marketing Authorization Procedure For Pharmaceuticals in Europe - Credevo ArticlesDocument12 pagesMarketing Authorization Procedure For Pharmaceuticals in Europe - Credevo ArticlesvinayNo ratings yet
- Historical SupplyDocument5 pagesHistorical Supplylara torricoNo ratings yet
- You - Stop When You See That Sign. You - Eat in Class. You - Keep Off The Grass! You - Take A Cough Syrup Once A Day. You - Tell My Secret To AnybodyDocument3 pagesYou - Stop When You See That Sign. You - Eat in Class. You - Keep Off The Grass! You - Take A Cough Syrup Once A Day. You - Tell My Secret To AnybodyDaniel D'AlessandroNo ratings yet
- Diagnosis For ParkinsonDocument7 pagesDiagnosis For ParkinsonAnna Mae SuminguitNo ratings yet
- The Status of PPFP in Bangladesh - WP 20 244 - D4I 1 1Document9 pagesThe Status of PPFP in Bangladesh - WP 20 244 - D4I 1 1Ridwanul MosrurNo ratings yet
- Research Note: K. Kumar, Debra Kemmler, and E. Riley HolmanDocument8 pagesResearch Note: K. Kumar, Debra Kemmler, and E. Riley HolmanHandoyo RianNo ratings yet
- Instructions On How To Properly Fill in The WAIRDocument17 pagesInstructions On How To Properly Fill in The WAIRRudy BancoroNo ratings yet
- Towards A Grand Convergence For Child Survival and HealthDocument78 pagesTowards A Grand Convergence For Child Survival and HealthNicholasNo ratings yet
- Personality Disorders in The Icd-11: Spanish Validation of The Picd and The Saspd in A Mixed Community and Clinical SampleDocument33 pagesPersonality Disorders in The Icd-11: Spanish Validation of The Picd and The Saspd in A Mixed Community and Clinical SampleBoskoBuhaNo ratings yet
- IRMA Pediatric Palliative CommunicationDocument40 pagesIRMA Pediatric Palliative CommunicationHelmi IrmawantyNo ratings yet
- Exam CDI 313Document4 pagesExam CDI 313Arianne FarnazoNo ratings yet
- BIO210 Chapter Summary 8Document6 pagesBIO210 Chapter Summary 8Rex BrazilNo ratings yet
- Boost Your Brainpower: Sistema Integrado de Gestión Procedimiento Ejecución de La Formación Profesional IntegralDocument7 pagesBoost Your Brainpower: Sistema Integrado de Gestión Procedimiento Ejecución de La Formación Profesional IntegralDiego Andres Pasachoa AmayaNo ratings yet
- Case Study 1Document6 pagesCase Study 1api-542345721No ratings yet
- Friendly House v. WhitingDocument27 pagesFriendly House v. WhitingLegal MomentumNo ratings yet
- Chapter I: Assessment: Comprehensive Nursing Process RubricDocument4 pagesChapter I: Assessment: Comprehensive Nursing Process RubricErika Cadawan100% (1)
- ClozapineDocument5 pagesClozapineANDREWNo ratings yet
- Dci 230030Document14 pagesDci 230030MARIA LEIVANo ratings yet
- Mukinge College of Nursing PHN JAN 2018: Port HealthDocument39 pagesMukinge College of Nursing PHN JAN 2018: Port HealthBa Mulenga100% (3)
- Safety Panelty Matrix For Contractor: SR - No Type of Safety Violation 1 Warning 2 Warning 3 WarningDocument2 pagesSafety Panelty Matrix For Contractor: SR - No Type of Safety Violation 1 Warning 2 Warning 3 WarningAejaz MujawarNo ratings yet
- General Hazards Tools and Equipment AHADocument1 pageGeneral Hazards Tools and Equipment AHAVijayakumarVageesanNo ratings yet
- Soal UTS Bahasa InggrisDocument3 pagesSoal UTS Bahasa InggrisPutri NayNo ratings yet
- Tamir Hands of ClitroidectomyDocument5 pagesTamir Hands of ClitroidectomyTechnic RealityNo ratings yet
- Annals of Tourism Research: Neil Carr (Associate Professor)Document2 pagesAnnals of Tourism Research: Neil Carr (Associate Professor)Alessandra Tarazona HiromotoNo ratings yet
- 1662725026318-1662725013173-Student Reg Form - BlankDocument4 pages1662725026318-1662725013173-Student Reg Form - BlankRuvarasheNo ratings yet
- Effects of Using Smartphones in Relation To Grade 12 Students Research of Estipona National High SchoolDocument2 pagesEffects of Using Smartphones in Relation To Grade 12 Students Research of Estipona National High SchoolTeacher GHENo ratings yet
- Professional EducationDocument54 pagesProfessional EducationJoshua AlibanNo ratings yet
- Module 2, Section 3 Reflection: The Sugar Film (2014) by Damon GarneauDocument3 pagesModule 2, Section 3 Reflection: The Sugar Film (2014) by Damon GarneauNicole Milan100% (3)