You might also like
- GRADE Guidelines: 10. Considering Resource Use and Rating The Quality of Economic EvidenceDocument12 pagesGRADE Guidelines: 10. Considering Resource Use and Rating The Quality of Economic EvidenceLourdesCarreraNo ratings yet
- Hex 19 483Document14 pagesHex 19 483LourdesCarreraNo ratings yet
- The Healthcare Complaints Analysis Tool: Development and Reliability Testing of A Method For Service Monitoring and Organisational LearningDocument10 pagesThe Healthcare Complaints Analysis Tool: Development and Reliability Testing of A Method For Service Monitoring and Organisational LearningLourdesCarreraNo ratings yet
- Patient Complaints in Healthcare Systems: A Systematic Review and Coding TaxonomyDocument12 pagesPatient Complaints in Healthcare Systems: A Systematic Review and Coding TaxonomyLourdesCarreraNo ratings yet
- Community Engagement and Its Impact On Child Health Disparities: Building Blocks, Examples, and ResourcesDocument11 pagesCommunity Engagement and Its Impact On Child Health Disparities: Building Blocks, Examples, and ResourcesLourdesCarreraNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NASKAH PUBLIKASI Fix PrintDocument16 pagesNASKAH PUBLIKASI Fix PrintNawawiNo ratings yet
- Probable Defense QuestionsDocument2 pagesProbable Defense Questionscayla mae carlos100% (1)
- 1479206723700-List of Approved Cancer HospitalsDocument8 pages1479206723700-List of Approved Cancer Hospitalslubx6xNo ratings yet
- 02-06-2021 HMB EnglishDocument63 pages02-06-2021 HMB EnglishMohammed IrfanNo ratings yet
- Final - Pfizer LOA To Issue With BLA Approval 08.23.21 - v2Document13 pagesFinal - Pfizer LOA To Issue With BLA Approval 08.23.21 - v2Tim Brown100% (3)
- Discharge PlanDocument2 pagesDischarge PlanJude Labajo100% (1)
- The Practice Specialty of Nursing Informatics (1/2)Document7 pagesThe Practice Specialty of Nursing Informatics (1/2)Wincy SalazarNo ratings yet
- Oral Cancer ScreeningDocument9 pagesOral Cancer ScreeningenNo ratings yet
- Iloilo Doctors' College College of Nursing: West Avenue, Molo, Iloilo CityDocument2 pagesIloilo Doctors' College College of Nursing: West Avenue, Molo, Iloilo CityAudrie Allyson GabalesNo ratings yet
- Kerangka Kerja Sistem Kesehatan (Who)Document15 pagesKerangka Kerja Sistem Kesehatan (Who)LipatriNo ratings yet
- Written Examination Handbook For General Dentistry May 2021-MinDocument20 pagesWritten Examination Handbook For General Dentistry May 2021-MinMuhammad Hassan memonNo ratings yet
- Registered Nurse Shortage Areas ReportDocument5 pagesRegistered Nurse Shortage Areas ReportAnthony WrightNo ratings yet
- Needle Stick Injuries Among Healthcare Waste Handlers in A Tertiary Care Hospital of DelhiDocument4 pagesNeedle Stick Injuries Among Healthcare Waste Handlers in A Tertiary Care Hospital of DelhiAdvanced Research PublicationsNo ratings yet
- Safder SMLE Seassion1 Infectious Diseases Part 1Document158 pagesSafder SMLE Seassion1 Infectious Diseases Part 1Sultan Al-OtaibiNo ratings yet
- Pharma Conpanies in Africa RegionDocument25 pagesPharma Conpanies in Africa RegionSiddhesh LawandeNo ratings yet
- Aids BrochureDocument2 pagesAids Brochureapi-340688414No ratings yet
- Conventional Treatment Options and Herbal Remedies For Male Infertility: AnDocument8 pagesConventional Treatment Options and Herbal Remedies For Male Infertility: AnNealNo ratings yet
- Osteonecrosis of The Femoral Head: Evaluation and TreatmentDocument10 pagesOsteonecrosis of The Femoral Head: Evaluation and TreatmentHector Ulises Quintanilla SotoNo ratings yet
- Study Guide For Postpartal Care-Module 7Document3 pagesStudy Guide For Postpartal Care-Module 7annyeong_123No ratings yet
- Nutritional Assessment in Critically Ill PatientsDocument19 pagesNutritional Assessment in Critically Ill PatientsSonia khanNo ratings yet
- INFS FTP Questionnaire 2Document4 pagesINFS FTP Questionnaire 2Abhishek ThakurNo ratings yet
- InfrastructureDocument4 pagesInfrastructureSachin AsherNo ratings yet
- Evidence Based Practice: Dorothea Orem's Self Care Deficit TheoryDocument37 pagesEvidence Based Practice: Dorothea Orem's Self Care Deficit TheoryVette Angelikka Dela CruzNo ratings yet
- Domains Domains: Mbbs Year 4C Curriculum Guide (Theme Iii/ Iv)Document2 pagesDomains Domains: Mbbs Year 4C Curriculum Guide (Theme Iii/ Iv)kanetrebleNo ratings yet
- Epidemiology of Digestive Helminthosis From Urban Area of Cluj-Napoca, RomaniaDocument9 pagesEpidemiology of Digestive Helminthosis From Urban Area of Cluj-Napoca, RomaniaΚΩΝΣΤΑΝΤΙΝΟΣ ΑΝΔΡΕΟΥNo ratings yet
- Company ProfileDocument3 pagesCompany ProfileJovan StoimenovskiNo ratings yet
- Antepartum AssessmentDocument14 pagesAntepartum Assessmentamena mahmoudNo ratings yet
- Emergency and Disaster NursingDocument9 pagesEmergency and Disaster NursingDempsey AlmirañezNo ratings yet
- NCMA 217 - Newborn Assessment Ma'am JhalDocument10 pagesNCMA 217 - Newborn Assessment Ma'am JhalMariah Blez BognotNo ratings yet
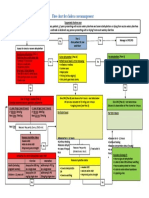
- Appendix 11. Flow Chart For Cholera Case ManagementDocument1 pageAppendix 11. Flow Chart For Cholera Case ManagementGerard Pio Wee100% (1)