You might also like
- Exercise Based Cardiac Rehabilitation For Adults After Heart Valve SurgeryDocument39 pagesExercise Based Cardiac Rehabilitation For Adults After Heart Valve Surgeryrima rizky nourliaNo ratings yet
- FCS (SA) Intermediate Paper 2 Blueprints 20-10-2019Document7 pagesFCS (SA) Intermediate Paper 2 Blueprints 20-10-2019Kishan NaiduNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- New Patient Questionnaire Physical Therapy: Chief ComplaintDocument4 pagesNew Patient Questionnaire Physical Therapy: Chief ComplaintAstonNo ratings yet
- Evaluation and Management of Small-Bowel Obstruction: An Eastern Association For The Surgery of Trauma Practice Management GuidelineDocument8 pagesEvaluation and Management of Small-Bowel Obstruction: An Eastern Association For The Surgery of Trauma Practice Management GuidelineAndreia MattiuciNo ratings yet
- Meta 6 - Khizar - 2023Document11 pagesMeta 6 - Khizar - 2023matheus.verasNo ratings yet
- Boom or Bust in OTDocument4 pagesBoom or Bust in OTSusan Ly VillalobosNo ratings yet
- Apendicitis Antibst NEJ 20Document2 pagesApendicitis Antibst NEJ 20Maria Gracia ChaconNo ratings yet
- Survival and Complications of Zygomatic Implants (PDFDrive)Document36 pagesSurvival and Complications of Zygomatic Implants (PDFDrive)Lê Minh KhôiNo ratings yet
- Prevention of Surgical Site Infections in Orthopaedic Surgery: A Synthesis of Current RecommendationsDocument16 pagesPrevention of Surgical Site Infections in Orthopaedic Surgery: A Synthesis of Current RecommendationsPankaj VatsaNo ratings yet
- Parker 2020Document6 pagesParker 2020QuiroprácticaParaTodosNo ratings yet
- Early Surgery Compared To Nonoperative ManagementDocument11 pagesEarly Surgery Compared To Nonoperative ManagementantoniowidiaNo ratings yet
- Terapia de Vacio en TraumaDocument11 pagesTerapia de Vacio en TraumaImha MikanersandsmashblastNo ratings yet
- Yao2017 Article DoesLaparoscopicAdhesiolysisDeDocument8 pagesYao2017 Article DoesLaparoscopicAdhesiolysisDeInamullah FurqanNo ratings yet
- Anterior Openbite Malocclusion in Adults Treatment Stability and Patient Satisfaction in National Dental Practice-Based Research Network PatientsDocument9 pagesAnterior Openbite Malocclusion in Adults Treatment Stability and Patient Satisfaction in National Dental Practice-Based Research Network PatientsScribd AccountNo ratings yet
- Ramirez 2013Document10 pagesRamirez 2013Nadia Farah FadhilaNo ratings yet
- The Rationale of Surgical Treatment in Pediatric Spine TuberculosisDocument6 pagesThe Rationale of Surgical Treatment in Pediatric Spine TuberculosisSpica KentNo ratings yet
- Clinical and Radiological Investigations To Predict Difficult Laparoscopic CholecystectomyDocument5 pagesClinical and Radiological Investigations To Predict Difficult Laparoscopic CholecystectomySuyash GhadgeNo ratings yet
- WarshawDocument11 pagesWarshawJuan RamirezNo ratings yet
- Association Between Orthodontic Treatment and Periodontal DiseasesDocument10 pagesAssociation Between Orthodontic Treatment and Periodontal DiseasesLalo MojicaNo ratings yet
- Efficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisChangjing ZhangNo ratings yet
- 2018 Lin G Laser Therapy For Treatment of Peri-Implant Mucositis and Peri-Implantitis - An American Academy of Periodontology Best Evidence Review.Document17 pages2018 Lin G Laser Therapy For Treatment of Peri-Implant Mucositis and Peri-Implantitis - An American Academy of Periodontology Best Evidence Review.iamkyantsaiNo ratings yet
- Ca Gastrico y EndosDocument27 pagesCa Gastrico y EndosIsraael JuuareezNo ratings yet
- Int Endodontic J - 2022 - Segura Egea - Impact of Systemic Health On Treatment Outcomes in Endodontics-1Document17 pagesInt Endodontic J - 2022 - Segura Egea - Impact of Systemic Health On Treatment Outcomes in Endodontics-1Nishant ChauhanNo ratings yet
- Tratamiento Esofago Cervical Lu, 2021Document9 pagesTratamiento Esofago Cervical Lu, 2021Carlos N. Rojas PuyolNo ratings yet
- Total or Partial Knee Replacement? Cost-Utility Analysis in Patients With Knee Osteoarthritis Based On A 2-Year Observational StudyDocument8 pagesTotal or Partial Knee Replacement? Cost-Utility Analysis in Patients With Knee Osteoarthritis Based On A 2-Year Observational StudyKevin FongNo ratings yet
- Tobert 2023Document8 pagesTobert 2023Will CKNo ratings yet
- A Systematic Review of The Single-Stage Treatment of Chronic OsteomyelitisDocument8 pagesA Systematic Review of The Single-Stage Treatment of Chronic Osteomyelitisrosa snakNo ratings yet
- BPH JournalDocument4 pagesBPH JournalTiffany ValentinaNo ratings yet
- Is Modern Perioperative Care Too Complicated For Surgeons?: ReferencesDocument2 pagesIs Modern Perioperative Care Too Complicated For Surgeons?: ReferencesHasriana BudimanNo ratings yet
- The Efficacy and Safety of Fire Needle For CervicaDocument5 pagesThe Efficacy and Safety of Fire Needle For CervicatrymybesthwlNo ratings yet
- Bhandari 2019Document37 pagesBhandari 2019Andrei SarmientoNo ratings yet
- Survival Prediction in Patients With Chronic LimbDocument18 pagesSurvival Prediction in Patients With Chronic LimbaizatamlikhaNo ratings yet
- Osteoporosis 2020Document46 pagesOsteoporosis 2020Angélica Montañez Robledo100% (1)
- What's New in Spine Surgery: Specialty UpdateDocument11 pagesWhat's New in Spine Surgery: Specialty UpdatePoliceNo ratings yet
- EzrzrzrDocument8 pagesEzrzrzrYoussef MotiaNo ratings yet
- HHS Public Access: A Protocol For The Management of Adhesive Small Bowel ObstructionDocument15 pagesHHS Public Access: A Protocol For The Management of Adhesive Small Bowel ObstructionMuhammad Aziz FirdausNo ratings yet
- Trauma, and Genital and Urethral Reconstruction: Re: Natural History of Low-Stage Urethral StricturesDocument2 pagesTrauma, and Genital and Urethral Reconstruction: Re: Natural History of Low-Stage Urethral StricturesWahyu IndraNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- Association Between Periodontal Health andDocument7 pagesAssociation Between Periodontal Health andTran DuongNo ratings yet
- Clinically Significant Outcomes After Meniscectomy 2019Document12 pagesClinically Significant Outcomes After Meniscectomy 2019asmaNo ratings yet
- Kees Tra 2014Document21 pagesKees Tra 2014Marco Antonio García LunaNo ratings yet
- Art 2Document21 pagesArt 2xdxdxdxdNo ratings yet
- El Tratamiento de La Obstrucción Del Intestino Delgado Con Un Fisioterapia Manual - Un Estudio de Eficacia Prospectivo.Document10 pagesEl Tratamiento de La Obstrucción Del Intestino Delgado Con Un Fisioterapia Manual - Un Estudio de Eficacia Prospectivo.DanielaNo ratings yet
- Shetty Et Al. 2008Document10 pagesShetty Et Al. 2008EmmanuelRajapandianNo ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- Clinical Study of Duodenal Perforation at Chief Jallahlone Government HospitalDocument1 pageClinical Study of Duodenal Perforation at Chief Jallahlone Government HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Patient Safety During Sedation by Anesthesia ProfeDocument8 pagesPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoNo ratings yet
- 190 Disc Repositioning Does It Really WorkDocument23 pages190 Disc Repositioning Does It Really WorkAngélica Valenzuela AndrighiNo ratings yet
- Collado Boira2021Document10 pagesCollado Boira2021Andreia LopesNo ratings yet
- Dong 2021Document23 pagesDong 2021jedan185No ratings yet
- Collagen Dressing in The Treatment of Diabetic Foot Ulcer: A Prospective, Randomized, Placebo-Controlled, Single-Center StudyDocument8 pagesCollagen Dressing in The Treatment of Diabetic Foot Ulcer: A Prospective, Randomized, Placebo-Controlled, Single-Center StudylatifaNo ratings yet
- Over Sem EsplintarDocument9 pagesOver Sem EsplintarClaudia BrilhanteNo ratings yet
- Radioembolization of Hepatic Malignancies - Background, Quality Improvement Guidelines, and Future DirectionsDocument15 pagesRadioembolization of Hepatic Malignancies - Background, Quality Improvement Guidelines, and Future DirectionsVeronica AlexanderNo ratings yet
- Informed Appropriate Imaging For Low Back Pain Management: A Narrative ReviewDocument14 pagesInformed Appropriate Imaging For Low Back Pain Management: A Narrative ReviewstephanNo ratings yet
- Orthopaedic Surgery - 2020 - Chen - Evaluation of Percutaneous Transforaminal Endoscopic Discectomy in The Treatment ofDocument9 pagesOrthopaedic Surgery - 2020 - Chen - Evaluation of Percutaneous Transforaminal Endoscopic Discectomy in The Treatment ofjy4r76dv6rNo ratings yet
- Perioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceDocument10 pagesPerioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceBRENDA VANESSA TREVIZO ESTRADANo ratings yet
- Choosing The Most Appropriate Biologic Therapy For Crohn's Disease According To Concomitant Extra-Intestinal Manifestations, Comorbidities, or Physiologic ConditionsDocument44 pagesChoosing The Most Appropriate Biologic Therapy For Crohn's Disease According To Concomitant Extra-Intestinal Manifestations, Comorbidities, or Physiologic ConditionsBernadett FarkasNo ratings yet
- File 712 20230127155855Document9 pagesFile 712 20230127155855Nakarit SangsirinawinNo ratings yet
- SASJS 88 508-515 wlsNAnDDocument8 pagesSASJS 88 508-515 wlsNAnDAnkita ChauhanNo ratings yet
- SR Diabetic Foot UlcerDocument11 pagesSR Diabetic Foot UlcerDeka AdeNo ratings yet
- sr10 260Document9 pagessr10 260Zulfikar BasriNo ratings yet
- Informed Consent in Elective and Emergency LaparosDocument2 pagesInformed Consent in Elective and Emergency LaparosFadi NasrallahNo ratings yet
- Agitacion Aguda PDFDocument9 pagesAgitacion Aguda PDFMaría José Díaz RojasNo ratings yet
- Pattern of Acute Intestinal Obstruction Is There A PDFDocument3 pagesPattern of Acute Intestinal Obstruction Is There A PDFMaría José Díaz RojasNo ratings yet
- Abdomen Agudo en El Adulto Mayor: Acute Abdomen in The ElderlyDocument8 pagesAbdomen Agudo en El Adulto Mayor: Acute Abdomen in The ElderlyMaría José Díaz RojasNo ratings yet
- 4 Jemds PDFDocument15 pages4 Jemds PDFMaría José Díaz RojasNo ratings yet
- Preoperative Skin PreparationDocument16 pagesPreoperative Skin PreparationSyahri DzikriNo ratings yet
- Dural Regeneration Matrix: U.S. Patent No. 5,997,895Document8 pagesDural Regeneration Matrix: U.S. Patent No. 5,997,895MasselliNo ratings yet
- Abdominal IncisionsDocument51 pagesAbdominal IncisionsFransisko ReinardNo ratings yet
- Pointers To Review Updated 2016Document18 pagesPointers To Review Updated 2016Rubelyn Arriola Nioko100% (1)
- Surgical PositionsDocument34 pagesSurgical PositionsArnel DominguezNo ratings yet
- Structura USMF, EnglezaDocument9 pagesStructura USMF, Englezadenis bosiiNo ratings yet
- (Journal of Neurosurgery - Spine) History and Advances in Spinal NeurosurgeryDocument11 pages(Journal of Neurosurgery - Spine) History and Advances in Spinal NeurosurgerycdsaludNo ratings yet
- Anesthesia For Maxillofacial ProcedureDocument90 pagesAnesthesia For Maxillofacial ProcedureAnirban Roy100% (1)
- AIA CorporateDocument4 pagesAIA CorporateWeng Meng VISTANo ratings yet
- Narayana Hrudayalaya Hospitals Research PaperDocument27 pagesNarayana Hrudayalaya Hospitals Research Paperapi-238825442No ratings yet
- Osteosarcoma 1Document9 pagesOsteosarcoma 1Md Ahsanuzzaman PinkuNo ratings yet
- Airways. DR HUSNIDocument89 pagesAirways. DR HUSNIFarah Fauziah RachmawatieNo ratings yet
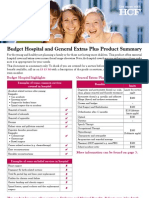
- Budget Hospital and General Extras Plus Product SummaryDocument4 pagesBudget Hospital and General Extras Plus Product SummaryJames SandersNo ratings yet
- Friday, 26 February 2016 12:00pm - 4:30pm Closing Date: 12 February 2015Document2 pagesFriday, 26 February 2016 12:00pm - 4:30pm Closing Date: 12 February 2015artemis_scribdNo ratings yet
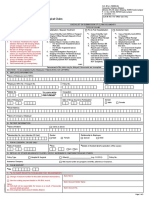
- Patient Face Sheet TemplateDocument5 pagesPatient Face Sheet TemplateAdrienn Krisztina VargaNo ratings yet
- 7 Tips On Avoiding Malpractice ClaimsDocument2 pages7 Tips On Avoiding Malpractice Claimsdardar8No ratings yet
- Ethical Issues in Palliative CareDocument16 pagesEthical Issues in Palliative CarevassalliNo ratings yet
- R e S H A P I NDocument32 pagesR e S H A P I Ncarla.garciaNo ratings yet
- 1647-Article Text-3369-1-10-20220320Document5 pages1647-Article Text-3369-1-10-20220320Eshan BhaleraoNo ratings yet
- Orthopedic Hospital Intro, O.T. & BMWDocument4 pagesOrthopedic Hospital Intro, O.T. & BMWjahanavi sharmaNo ratings yet
- Tahbso ArticleDocument4 pagesTahbso ArticleAlianna Kristine OhNo ratings yet
- Protesis Columna Roi-ADocument36 pagesProtesis Columna Roi-AValery Poccomo SotoNo ratings yet
- proGAV2.0 TA013871 SOP-AIC-5001399Document22 pagesproGAV2.0 TA013871 SOP-AIC-5001399LouisWangNo ratings yet
- Awad 2020Document13 pagesAwad 2020Doctor's BettaNo ratings yet
- Shaft of Humerus Fracture Managed by Anteromedial Plating Through Anterolateral ApproachDocument5 pagesShaft of Humerus Fracture Managed by Anteromedial Plating Through Anterolateral ApproachMukesh KumarNo ratings yet
- Robotic SurgeryDocument21 pagesRobotic SurgerysayyanNo ratings yet
- Herrmann, Galle 2011 - Retrospective Surgery StudyDocument8 pagesHerrmann, Galle 2011 - Retrospective Surgery StudyBeehappy.grNo ratings yet