You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
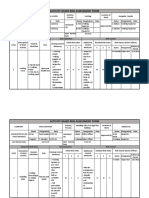
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- ST Bridget's DebriefDocument8 pagesST Bridget's DebriefSri NarendiranNo ratings yet
- Resume Danika AcostaDocument2 pagesResume Danika Acostaapi-508877504No ratings yet
- Lessons Learned From The Dog GenomeDocument11 pagesLessons Learned From The Dog GenomebellonicoNo ratings yet
- The Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesDocument8 pagesThe Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesLwsynergylab OfficialNo ratings yet
- Tennessee Hazard Mitigation Plan 2018 FINALDocument388 pagesTennessee Hazard Mitigation Plan 2018 FINALAnonymous GF8PPILW5100% (1)
- Pbs Register of SponsorsDocument1,727 pagesPbs Register of SponsorsZaili KastamNo ratings yet
- English Test: Surname: Points: /100Document3 pagesEnglish Test: Surname: Points: /100Елена Китанова ЃошевскаNo ratings yet
- Full Length Research Article: ISSN: 2230-9926Document5 pagesFull Length Research Article: ISSN: 2230-9926Nisarg SutharNo ratings yet
- Self HypnosisDocument56 pagesSelf HypnosisMarinNo ratings yet
- Say No To PlasticDocument28 pagesSay No To Plasticpavithra nirmalaNo ratings yet
- Literature Review of Quantitative StudiesDocument5 pagesLiterature Review of Quantitative Studiesd0vidihujam3100% (1)
- Ventilator Circuit Filter and Humidification Setup July 2021 1c6nn8Document4 pagesVentilator Circuit Filter and Humidification Setup July 2021 1c6nn8Hubert Jiménez GarciaNo ratings yet
- Contractor Safety Rules PDFDocument10 pagesContractor Safety Rules PDFKEERTHI INDUSTRIESNo ratings yet
- Backwardness of Women Leads To Backwardness of The Nation PDFDocument3 pagesBackwardness of Women Leads To Backwardness of The Nation PDFMuhammad ShahZadNo ratings yet
- Hong Leong TakafulDocument43 pagesHong Leong TakafulfarahzatulizzaNo ratings yet
- Lightner Witmer and The First 100 Years of Clinical PsychologyDocument4 pagesLightner Witmer and The First 100 Years of Clinical PsychologyjuaromerNo ratings yet
- Narrativa Analysis Catherine - Kohler - Riessman PDFDocument9 pagesNarrativa Analysis Catherine - Kohler - Riessman PDFJéssica FigueiredoNo ratings yet
- Home Care Catalogue UK Edition 4 Web PDFDocument60 pagesHome Care Catalogue UK Edition 4 Web PDFmanuales tecnicosNo ratings yet
- Prep ColonosDocument13 pagesPrep ColonosKarlNo ratings yet
- Arntz 1999 Childhood Imagery Rescripting Paper PDFDocument26 pagesArntz 1999 Childhood Imagery Rescripting Paper PDFelliotNo ratings yet
- Reflection Paper MULANAYDocument2 pagesReflection Paper MULANAYRob40% (5)
- Tratament Diuretic in Insuficienta CardiacaDocument19 pagesTratament Diuretic in Insuficienta CardiacaOlga HMNo ratings yet
- Physical Education: Quarter 4 - Module 1 Week 1: FITT PrincipleDocument19 pagesPhysical Education: Quarter 4 - Module 1 Week 1: FITT PrincipleTrexia SingsonNo ratings yet
- Mirzi S. Turbolencia,: Curriculum VitaeDocument2 pagesMirzi S. Turbolencia,: Curriculum VitaeChester KyleNo ratings yet
- Provide First AidDocument3 pagesProvide First AidluviumNo ratings yet
- Phyto 2Document1 pagePhyto 2Farhan AshrafNo ratings yet
- Anti-Inflammatory Diet: What Is Inflammation?Document13 pagesAnti-Inflammatory Diet: What Is Inflammation?Perrela PerrelaNo ratings yet
- Below Knee AmputationDocument6 pagesBelow Knee AmputationAmacayoNo ratings yet
- Table of Specification For Second Periodical Test in Mapeh IvDocument4 pagesTable of Specification For Second Periodical Test in Mapeh IvJENNIFER SERVONo ratings yet