You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
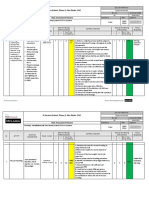
- Risk Assessment For Installation of Fire Alarm System & PAVA SystemDocument11 pagesRisk Assessment For Installation of Fire Alarm System & PAVA SystemAnandu Ashokan88% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tummy Time Rolling and CrawlingDocument20 pagesTummy Time Rolling and CrawlingIndah Yulantari100% (1)
- NeoReviews January 2023Document58 pagesNeoReviews January 2023Ronald MHNo ratings yet
- Workbook 031512 With Cover PDFDocument197 pagesWorkbook 031512 With Cover PDFIndah Yulantari100% (2)
- Pain The Science of SufferingDocument185 pagesPain The Science of SufferingAlejandroNo ratings yet
- Chum-Health-Sheets-531-1-Taking-Care-Of-My Scars-With-MassageDocument4 pagesChum-Health-Sheets-531-1-Taking-Care-Of-My Scars-With-MassageIndah YulantariNo ratings yet
- DLP IN HEALTH-Gr.9Document7 pagesDLP IN HEALTH-Gr.9Aliah Mae MontanoNo ratings yet
- Lower Limb Neurological Examination OSCE GuideDocument15 pagesLower Limb Neurological Examination OSCE GuideLeen abusarhanNo ratings yet
- Contusions May Coalesce To Form An Intracerebral Hematoma. TBI/ICH - HTMLDocument17 pagesContusions May Coalesce To Form An Intracerebral Hematoma. TBI/ICH - HTMLEsterida Simanjuntak100% (1)
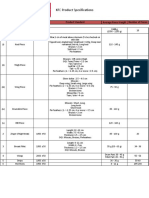
- KFC Poultry Product SpecificationsDocument1 pageKFC Poultry Product SpecificationsInaam Ur RehmanNo ratings yet
- Confounding Variables in Epidemiologic Studies: Basics and BeyondDocument10 pagesConfounding Variables in Epidemiologic Studies: Basics and BeyondIndah YulantariNo ratings yet
- Measurement and EvaluationDocument21 pagesMeasurement and EvaluationIndah YulantariNo ratings yet
- Training For Balance and Improved Muscle Coordination Using The BosuDocument2 pagesTraining For Balance and Improved Muscle Coordination Using The BosuIndah YulantariNo ratings yet
- Ou Yang2017Document10 pagesOu Yang2017Indah YulantariNo ratings yet
- Treatment of Extensive Postburn Deformities Using Extralarge Sheets of Full Thickness Skin GraftsDocument8 pagesTreatment of Extensive Postburn Deformities Using Extralarge Sheets of Full Thickness Skin GraftsIndah YulantariNo ratings yet
- The Technique of Physical Rehabilitation in ClubfoDocument11 pagesThe Technique of Physical Rehabilitation in ClubfoIndah YulantariNo ratings yet
- Case Study of Physiotherapy Treatment of A Patient Following Total Knee ReplacementDocument105 pagesCase Study of Physiotherapy Treatment of A Patient Following Total Knee ReplacementIndah YulantariNo ratings yet
- Effect of Physical Therapy Frequency On Gross Moto PDFDocument4 pagesEffect of Physical Therapy Frequency On Gross Moto PDFIndah YulantariNo ratings yet
- 189-198 FukatoVol8No3 PDFDocument10 pages189-198 FukatoVol8No3 PDFIndah YulantariNo ratings yet
- Jospt 2006 2198Document9 pagesJospt 2006 2198Indah YulantariNo ratings yet
- Pulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionDocument7 pagesPulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionIndah YulantariNo ratings yet
- Motor Assessment in Patients With Duchenne MusculaDocument6 pagesMotor Assessment in Patients With Duchenne MusculaIndah YulantariNo ratings yet
- Effects of An Exercise Program On Diastasis Recti in WomenDocument10 pagesEffects of An Exercise Program On Diastasis Recti in WomenIndah YulantariNo ratings yet
- IJHSRUN CaseReportDocument5 pagesIJHSRUN CaseReportIndah YulantariNo ratings yet
- Value of Transcutaneous Electric Nerve StimulationDocument5 pagesValue of Transcutaneous Electric Nerve StimulationIndah YulantariNo ratings yet
- Manual Esab 352 CVDocument28 pagesManual Esab 352 CVJaSon MadridNo ratings yet
- Unit 8Document13 pagesUnit 8Huy NguyenNo ratings yet
- Sample Medical Malpractice ComplaintDocument3 pagesSample Medical Malpractice ComplaintNestor RiveroNo ratings yet
- Anatomy Lecture 13 - Anatomic Topographic Regions - PerineumDocument25 pagesAnatomy Lecture 13 - Anatomic Topographic Regions - PerineumCIPSITNo ratings yet
- Lesson 3B VolleyballDocument2 pagesLesson 3B VolleyballRuby BalisiNo ratings yet
- Anatomi EoDocument13 pagesAnatomi EoadindaNo ratings yet
- Spinal Cord Injury Oleh DR Cok SP - OtDocument50 pagesSpinal Cord Injury Oleh DR Cok SP - OtPipit ArikaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Chikuda 2021 Oi 210953 1639158704.75905Document13 pagesChikuda 2021 Oi 210953 1639158704.75905Neda PiratvisuthNo ratings yet
- Ebook Grainger Allisons Diagnostic Radiology Essentials PDF Full Chapter PDFDocument67 pagesEbook Grainger Allisons Diagnostic Radiology Essentials PDF Full Chapter PDFlisa.dolan637100% (25)
- Chest TraumaDocument62 pagesChest TraumaayouNo ratings yet
- JageshwarDocument1 pageJageshwarrajeshsaloaNo ratings yet
- Swallowing Rehabilitation Following Spinal Injury A Case SeriesDocument12 pagesSwallowing Rehabilitation Following Spinal Injury A Case SeriesniekoNo ratings yet
- Locomotion and MovementDocument3 pagesLocomotion and MovementYouTutor PSNo ratings yet
- Midterm Risk ModuleDocument16 pagesMidterm Risk ModuleJessa CapangpanganNo ratings yet
- Arches of Foot: DR M Idris SiddiquiDocument22 pagesArches of Foot: DR M Idris SiddiquiSivabharathi SivanandamNo ratings yet
- Ehler Danlos SyndromeDocument3 pagesEhler Danlos Syndromeandreas kevinNo ratings yet
- Anatomy Image Bank Edition 2 Updated Upto NEET PG 21Document130 pagesAnatomy Image Bank Edition 2 Updated Upto NEET PG 21Yogaabirami AbiNo ratings yet
- Anatomy TopoDocument62 pagesAnatomy TopoDoina GoreanuNo ratings yet
- Police DogsDocument8 pagesPolice Dogsserbi1962No ratings yet
- Basic Knee Arthroscopy Part 2Document2 pagesBasic Knee Arthroscopy Part 2Diego BellingNo ratings yet
- Skull 2Document34 pagesSkull 2saifNo ratings yet
- Lfi 2018 004Document1 pageLfi 2018 004Nelz PelaezNo ratings yet