You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MoH Digital Health Strategy UpdateDocument39 pagesMoH Digital Health Strategy UpdateAldrinNo ratings yet
- MBBS Final Year Send Up Examination 2020Document26 pagesMBBS Final Year Send Up Examination 2020Ali SohailNo ratings yet
- Carpal Tunnel SyndromeDocument13 pagesCarpal Tunnel SyndromeWalid SolimanNo ratings yet
- NCP LymphomaDocument4 pagesNCP LymphomaRene John Francisco100% (2)
- Historical Evolution of NursingDocument33 pagesHistorical Evolution of NursingAnuchithra Radhakrishnan100% (1)
- Nursing Care Plan Ovarian CancerDocument2 pagesNursing Care Plan Ovarian CancerKathleen Dimacali100% (1)
- PM 7379 119 119680-Di6h3qgi4xDocument169 pagesPM 7379 119 119680-Di6h3qgi4xAldrinNo ratings yet
- Malaria in The Who European Region: Key MessagesDocument8 pagesMalaria in The Who European Region: Key MessagesAldrinNo ratings yet
- Philippines: Situation Report 18Document6 pagesPhilippines: Situation Report 18AldrinNo ratings yet
- Hero BACK SCHOOL-CHECKLIST PDFDocument1 pageHero BACK SCHOOL-CHECKLIST PDFAldrinNo ratings yet
- Checklist Tool GuideDocument2 pagesChecklist Tool GuideAldrinNo ratings yet
- COVID-19 Safety Guide For Healthcare Workers Version 3.0Document40 pagesCOVID-19 Safety Guide For Healthcare Workers Version 3.0Aldrin100% (1)
- Preparing School Buildings For Reopening After COVID-19: The Safe School SixDocument1 pagePreparing School Buildings For Reopening After COVID-19: The Safe School SixAldrinNo ratings yet
- Facts Achievements Layout - Final - Email (SQ)Document21 pagesFacts Achievements Layout - Final - Email (SQ)AldrinNo ratings yet
- Page 1 of 7Document7 pagesPage 1 of 7AldrinNo ratings yet
- Saudi Moh Protocol For Patients Suspected Of/Confirmed With Covid-19Document15 pagesSaudi Moh Protocol For Patients Suspected Of/Confirmed With Covid-19AldrinNo ratings yet
- Philippines: Situation Report 38Document8 pagesPhilippines: Situation Report 38AldrinNo ratings yet
- Potential Customer President of The Company Certification Auditing, Consulting and Training AdminDocument1 pagePotential Customer President of The Company Certification Auditing, Consulting and Training AdminAldrinNo ratings yet
- Step 3: Processes of The OH&S Management System: For Use Internally in The OrganizationDocument1 pageStep 3: Processes of The OH&S Management System: For Use Internally in The OrganizationAldrinNo ratings yet
- How To Document A NonconformityDocument1 pageHow To Document A NonconformityAldrinNo ratings yet
- Step 3: Processes of The OH&S Management System: For Use Internally in The OrganizationDocument1 pageStep 3: Processes of The OH&S Management System: For Use Internally in The OrganizationAldrinNo ratings yet
- Correction Report: Inspection Number Correction Contractor Date Date Inspected by StatusDocument2 pagesCorrection Report: Inspection Number Correction Contractor Date Date Inspected by StatusAldrinNo ratings yet
- Steps For Implementing ISO 45001 SimplifiedDocument1 pageSteps For Implementing ISO 45001 SimplifiedAldrinNo ratings yet
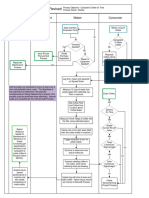
- Creation of A Cup of Coffee - Revised: Maintenance Consumer Maker ProcurementDocument1 pageCreation of A Cup of Coffee - Revised: Maintenance Consumer Maker ProcurementAldrinNo ratings yet
- Color Splash Slides: Sample Text Sample TextDocument5 pagesColor Splash Slides: Sample Text Sample TextAldrinNo ratings yet
- 1.1a Buildings and Floors Inspection ReportDocument1 page1.1a Buildings and Floors Inspection ReportAldrinNo ratings yet
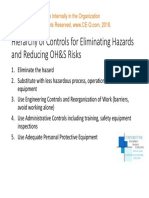
- Hierarchy of Controls of ISO 45001Document1 pageHierarchy of Controls of ISO 45001AldrinNo ratings yet
- To, Vivian, PA PDFDocument22 pagesTo, Vivian, PA PDFVivianToNo ratings yet
- Sialolithiasis: Radiological Diagnosis and Treatment: NovemberDocument33 pagesSialolithiasis: Radiological Diagnosis and Treatment: NovemberAciih HeHoNo ratings yet
- Doh Programs First 1000 Days Ni BabyDocument65 pagesDoh Programs First 1000 Days Ni BabyjpnachorNo ratings yet
- Pharmacology LogbookDocument4 pagesPharmacology LogbookMahmudul Hasan SazibNo ratings yet
- Jurnal Kennel CoughDocument12 pagesJurnal Kennel Coughtrisnaput3No ratings yet
- Toxoplasmosis and LaishmaniosisDocument49 pagesToxoplasmosis and LaishmaniosisTarikNo ratings yet
- Intellectual Journey EssayDocument7 pagesIntellectual Journey Essayapi-538926439No ratings yet
- Guideline For Field Visit ReportDocument4 pagesGuideline For Field Visit Reportmdkasim904No ratings yet
- Unicompartmental Knee ArthroplastyDocument10 pagesUnicompartmental Knee Arthroplastycronoss21No ratings yet
- Blood Donation Frequently Asked QuestionsDocument3 pagesBlood Donation Frequently Asked QuestionsGrace ThairuNo ratings yet
- Abune Gorgorious Schools Lebu Branch: Grade 6 Su. ScienceDocument7 pagesAbune Gorgorious Schools Lebu Branch: Grade 6 Su. ScienceBekalu BimrewNo ratings yet
- RSAL - Hipoksia JaninDocument16 pagesRSAL - Hipoksia JaninLoserlikemeNo ratings yet
- Gtoz (Getting To Zero) : Zero New Hiv Infection Zero Aids Related Deaths Zero DiscriminationDocument32 pagesGtoz (Getting To Zero) : Zero New Hiv Infection Zero Aids Related Deaths Zero DiscriminationSheyPNNo ratings yet
- Biosafty One ChapterDocument20 pagesBiosafty One ChaptertofakalidNo ratings yet
- Physiotherapy2019 ScientificProgramDocument4 pagesPhysiotherapy2019 ScientificProgramCristinaMolasNo ratings yet
- Drugs and Alcohol Questions For Tests and Worksheets - Page 10Document3 pagesDrugs and Alcohol Questions For Tests and Worksheets - Page 10Takesure MarizaniNo ratings yet
- Vaccination Contre La Covid-19: Voici Le CalendrierDocument6 pagesVaccination Contre La Covid-19: Voici Le CalendrierDefimedia100% (1)
- Cancer Lesson Plan - Tutor1Document7 pagesCancer Lesson Plan - Tutor1ta CNo ratings yet
- Gkha 2019Document172 pagesGkha 2019Elena CuibanNo ratings yet
- TB Statistics in The PhilippinesDocument4 pagesTB Statistics in The PhilippinesJoy LualhatiNo ratings yet
- English Presentation!Document13 pagesEnglish Presentation!German AcostaNo ratings yet
- Petersen 2001Document30 pagesPetersen 2001Bianca MagnelliNo ratings yet
- NHS FPX 6008 Assessment 1 Identifying A Local Health Care Economic IssueDocument6 pagesNHS FPX 6008 Assessment 1 Identifying A Local Health Care Economic Issuejoohnsmith070No ratings yet
- APA TemplateDocument5 pagesAPA TemplateDaud AhmadNo ratings yet
- Repertorial Approach of Diabetes MellitusDocument4 pagesRepertorial Approach of Diabetes MellitusHomoeopathic Pulse100% (1)