You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Inexpensive FIA Method To Determine Trace Levels of Imazapyr by UV-detection Enhanced With Electrochemical PolarizationDocument8 pagesInexpensive FIA Method To Determine Trace Levels of Imazapyr by UV-detection Enhanced With Electrochemical PolarizationKarin AdraiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On The Sound Field From A Source Moving Above Non - 2020 - Journal of Sound andDocument20 pagesOn The Sound Field From A Source Moving Above Non - 2020 - Journal of Sound andTaniaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 1 s2.0 S0022460X19305474 MainDocument11 pages1 s2.0 S0022460X19305474 MainKarin AdraiNo ratings yet
- Crack The Core Exam - Volume 2 4th PDFDocument508 pagesCrack The Core Exam - Volume 2 4th PDFQuỳnh Trâm86% (7)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Nanoparticles: Properties, Applications and Toxicities: Arabian Journal of ChemistryDocument24 pagesNanoparticles: Properties, Applications and Toxicities: Arabian Journal of Chemistryrazor926No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Caesarian SectionDocument26 pagesCaesarian SectionKarin AdraiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Quantifying Normal Human Brain Metabolism Using Hyperpolarized (1-13C) Pyruvate and Magnetic Resonance Imaging - Elsevier Enhanced ReaderDocument9 pagesQuantifying Normal Human Brain Metabolism Using Hyperpolarized (1-13C) Pyruvate and Magnetic Resonance Imaging - Elsevier Enhanced ReaderKarin AdraiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Synthesis, Anti-Tuberculosis Activity and QSARstudy of 2,4-Diarylquinolines and Analogouspolycyclic DerivativesDocument14 pagesSynthesis, Anti-Tuberculosis Activity and QSARstudy of 2,4-Diarylquinolines and Analogouspolycyclic DerivativeskostNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- מאמר על מצלמה תרמית אחרי רה-וסקולריציהDocument4 pagesמאמר על מצלמה תרמית אחרי רה-וסקולריציהKarin AdraiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- WelcomeDocument5 pagesWelcomeCatNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- ראשון קריןDocument9 pagesראשון קריןKarin AdraiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Carcinogen Es IsDocument33 pagesCarcinogen Es IsKarin AdraiNo ratings yet
- vascular surgery ספר פשוט PDFDocument92 pagesvascular surgery ספר פשוט PDFKarin AdraiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- WelcomeDocument5 pagesWelcomeCatNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Transient Ischemic Attack: Every Minute CountsDocument54 pagesTransient Ischemic Attack: Every Minute CountsKarin AdraiNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Create A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouDocument6 pagesCreate A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouKarin AdraiNo ratings yet
- Inflammatory Bowl DiseaseDocument23 pagesInflammatory Bowl DiseaseKarin AdraiNo ratings yet
- ABB DisordersDocument27 pagesABB DisordersKarin AdraiNo ratings yet
- GeneticsDocument31 pagesGeneticsKarin AdraiNo ratings yet
- Create A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouDocument6 pagesCreate A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouKarin AdraiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lecture Notes First Semester Yr 2 BPham BMLS BDSDocument57 pagesLecture Notes First Semester Yr 2 BPham BMLS BDSKarin AdraiNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Summary of ECG AbnormalitiesDocument7 pagesSummary of ECG AbnormalitiesKarin AdraiNo ratings yet
- Learn To Hear The Voice of GodDocument110 pagesLearn To Hear The Voice of Godtrue prophet100% (1)
- Annual Report 18Document363 pagesAnnual Report 18Safeer UllahNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Technical Information System Overview Prosafe-Com 3.00 Prosafe-ComDocument49 pagesTechnical Information System Overview Prosafe-Com 3.00 Prosafe-Comshekoofe danaNo ratings yet
- WISECO 2011 Complete CatalogDocument131 pagesWISECO 2011 Complete CatalogfishuenntNo ratings yet
- Technology Class ResumeDocument4 pagesTechnology Class Resumeapi-259588430No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- High Speed Board Design: Signal Integrity AnalysisDocument35 pagesHigh Speed Board Design: Signal Integrity Analysissrikanth chundiNo ratings yet
- Gamble V Tyson MSJDocument41 pagesGamble V Tyson MSJTHROnlineNo ratings yet
- 01 - PV - RESCO 1d Workshop - S1 PDFDocument61 pages01 - PV - RESCO 1d Workshop - S1 PDFDeasy KurniawatiNo ratings yet
- Forecast Time Series-NotesDocument138 pagesForecast Time Series-NotesflorinNo ratings yet
- Management Theory and Practice: Methods of Performance AppraisalDocument3 pagesManagement Theory and Practice: Methods of Performance AppraisalRadha maiNo ratings yet
- Xt600e 3tb-3uw 90-95Document46 pagesXt600e 3tb-3uw 90-95Kenneth SynnesNo ratings yet
- SecASC - M02 - Azure Security Center Setup and ConfigurationDocument53 pagesSecASC - M02 - Azure Security Center Setup and ConfigurationGustavo WehdekingNo ratings yet
- FacebookH Cking 1 3 (SFILEDocument10 pagesFacebookH Cking 1 3 (SFILEFitra AkbarNo ratings yet
- ForwardMails PDFDocument7 pagesForwardMails PDFJesús Ramón Romero EusebioNo ratings yet
- Huang V Tesla State of Calif 20190430Document20 pagesHuang V Tesla State of Calif 20190430jonathan_skillings100% (1)
- MKTG 2126 - Assignment 3Document2 pagesMKTG 2126 - Assignment 3omar mcintoshNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- IGNOU MBA MS-11 Solved AssignmentDocument5 pagesIGNOU MBA MS-11 Solved AssignmenttobinsNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- Map Project Rubric 2018Document2 pagesMap Project Rubric 2018api-292774341No ratings yet
- DOJ OIG Issues 'Fast and Furious' ReportDocument512 pagesDOJ OIG Issues 'Fast and Furious' ReportFoxNewsInsiderNo ratings yet
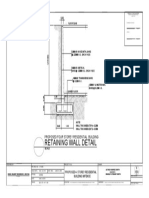
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- Quantification Skills in The Construction IndustryDocument34 pagesQuantification Skills in The Construction IndustryBRGRNo ratings yet
- Fellowship in OncotherapeutDocument3 pagesFellowship in OncotherapeutNayan ChaudhariNo ratings yet
- Effect of Upstream Dam Geometry On Peak Discharge During Overtopping Breach in Noncohesive Homogeneous Embankment Dams Implications For Tailings DamsDocument22 pagesEffect of Upstream Dam Geometry On Peak Discharge During Overtopping Breach in Noncohesive Homogeneous Embankment Dams Implications For Tailings DamsHelvecioNo ratings yet
- BTEC International Level 3 IT Pearson Set Assignment Unit 11 Cyber SecurityDocument8 pagesBTEC International Level 3 IT Pearson Set Assignment Unit 11 Cyber SecurityGergana Stamenova100% (1)
- Taylor Introms11GE PPT 03Document40 pagesTaylor Introms11GE PPT 03hddankerNo ratings yet
- Plant Disease Detection Using Deep LearningDocument5 pagesPlant Disease Detection Using Deep LearningIJRASETPublicationsNo ratings yet
- Little ThingsDocument3 pagesLittle ThingszwartwerkerijNo ratings yet
- 2iccas2005 Paper 377Document5 pages2iccas2005 Paper 377Cristian BandilaNo ratings yet
- Batt ChargerDocument2 pagesBatt Chargerdjoko witjaksonoNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)