You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- National School Building Inventory (NSBI) Encoding For SY 2021-2022Document31 pagesNational School Building Inventory (NSBI) Encoding For SY 2021-2022Renato Rivera100% (1)
- Lezione Argiolu - Master Roma3!3!12-2010 - Test Di Application SecurityDocument26 pagesLezione Argiolu - Master Roma3!3!12-2010 - Test Di Application SecurityWB_YeatsNo ratings yet
- Project On Brand Awareness of ICICI Prudential by SajadDocument99 pagesProject On Brand Awareness of ICICI Prudential by SajadSajadul Ashraf71% (7)
- XXX RadiographsDocument48 pagesXXX RadiographsJoseph MidouNo ratings yet
- Pricelist Jan 2023Document7 pagesPricelist Jan 2023Rahmat FadilNo ratings yet
- Analisis Pendapatan Dan Kesejahteraan Rumah Tangga Nelayan Cumi-Cumi Di Desa Sukajaya Lempasing Kecamatan Teluk Pandan Kabupaten PesawaranDocument12 pagesAnalisis Pendapatan Dan Kesejahteraan Rumah Tangga Nelayan Cumi-Cumi Di Desa Sukajaya Lempasing Kecamatan Teluk Pandan Kabupaten PesawaranAldy Suryo KuncoroNo ratings yet
- Media DRIVEON Vol25 No2Document21 pagesMedia DRIVEON Vol25 No2Nagenthara PoobathyNo ratings yet
- LTE Radio Network Design Guideline (FDD)Document33 pagesLTE Radio Network Design Guideline (FDD)Tri Frida NingrumNo ratings yet
- Ashirvad SWR and SWR PLUS - Price List - 02nd April 2022Document14 pagesAshirvad SWR and SWR PLUS - Price List - 02nd April 2022Magnum ConstructionsNo ratings yet
- FEDocument20 pagesFEKenadid Ahmed OsmanNo ratings yet
- Notes in Judicial AffidavitDocument11 pagesNotes in Judicial AffidavitguibonganNo ratings yet
- Revised Procedural Manual On Hazardous Waste Management (Revised DAO 04-36) I CONTENTS Chapter Page PDFDocument53 pagesRevised Procedural Manual On Hazardous Waste Management (Revised DAO 04-36) I CONTENTS Chapter Page PDFdennisNo ratings yet
- Bảo MậtDocument2 pagesBảo MậtMinh Nghia PhamNo ratings yet
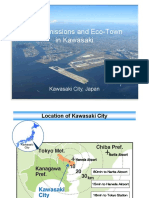
- 03 Zero Emissions and Eco-Town in KawasakiDocument21 pages03 Zero Emissions and Eco-Town in KawasakiAlwi AmarNo ratings yet
- The US Navy - Fact File - MQ-8C Fire ScoutDocument2 pagesThe US Navy - Fact File - MQ-8C Fire ScoutAleksei KarpaevNo ratings yet
- Urban Issues: Rio Case StudyDocument4 pagesUrban Issues: Rio Case Studyxbox pro hiNo ratings yet
- Basic CommandsDocument40 pagesBasic CommandsPrashant RaiNo ratings yet
- 150 67-Eg1Document104 pages150 67-Eg1rikoNo ratings yet
- Ranbaxy Acquisition by DaiichiDocument9 pagesRanbaxy Acquisition by Daiichirupe59No ratings yet
- Cronbach's AlphaDocument4 pagesCronbach's AlphaHeide Orevillo Apa-apNo ratings yet
- Opposition To Motion For Judgment On PleadingsDocument31 pagesOpposition To Motion For Judgment On PleadingsMark Jaffe100% (1)
- Chennai CMDA Master Plan 2026 Volume 3 Sectorial BackgroundDocument270 pagesChennai CMDA Master Plan 2026 Volume 3 Sectorial BackgroundMalathi Kathirvel100% (1)
- Corality ModelOff Sample Answer Hard TimesDocument81 pagesCorality ModelOff Sample Answer Hard TimesserpepeNo ratings yet
- Soal Ujian SmaDocument26 pagesSoal Ujian SmaAyu RiskyNo ratings yet
- Best of SEO#1 SEO Training & Content Marketing Course 2022Document2 pagesBest of SEO#1 SEO Training & Content Marketing Course 2022Oscar MascarenoNo ratings yet
- Lust V Animal Logic MSJ OppositionDocument34 pagesLust V Animal Logic MSJ OppositionTHROnlineNo ratings yet
- Sample Lesson Plan Baking Tools and EquipmentDocument3 pagesSample Lesson Plan Baking Tools and EquipmentJoenel PabloNo ratings yet
- OEM - Fuel Manager Brand Cross Reference P/Ns For Service Filter Elements 99642 - January 2006Document6 pagesOEM - Fuel Manager Brand Cross Reference P/Ns For Service Filter Elements 99642 - January 2006Miguel RojasNo ratings yet
- Epsilon Range Bomba HorizontalDocument8 pagesEpsilon Range Bomba HorizontalsalazarafaelNo ratings yet
- GROZ Tools & Equipment 2018Document3 pagesGROZ Tools & Equipment 2018ayush bansalNo ratings yet