You might also like
- Nursing Care Plan For Patients With FractureDocument3 pagesNursing Care Plan For Patients With Fracture_cezca_89% (168)
- Savage Worlds MLP EditionDocument66 pagesSavage Worlds MLP EditionCarsten_Curren_7854100% (8)
- Gordon's Functional Health Pattern For Geriatric ClientsDocument8 pagesGordon's Functional Health Pattern For Geriatric ClientsGEN ERIGBUAGASNo ratings yet
- Readiness Nursing Care PlanDocument9 pagesReadiness Nursing Care PlanFEIYEN ZhuoNo ratings yet
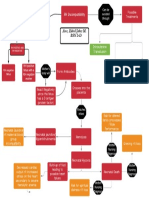
- Basic Concept Map - RH IncompatibilityDocument1 pageBasic Concept Map - RH IncompatibilityTechnoShindoNo ratings yet
- Lonzaga Assessment PDFDocument7 pagesLonzaga Assessment PDFNiño Naryana Luke PanchoNo ratings yet
- Our Iceberg Is MeltingDocument5 pagesOur Iceberg Is Meltingyogeshdhuri22No ratings yet
- Chapter - 6 Performance ManagementDocument34 pagesChapter - 6 Performance ManagementPreeti BhaskarNo ratings yet
- 324 (High Court) Muhammas SaifDocument17 pages324 (High Court) Muhammas SaifHiskeel AhmadNo ratings yet
- Goboy - Risk For Infection NCPDocument3 pagesGoboy - Risk For Infection NCPLouise GermaineNo ratings yet
- Vii. NCPDocument4 pagesVii. NCPmariaNo ratings yet
- 1st Level Assessment JAVIER FOR STA CRUZ CASEDocument4 pages1st Level Assessment JAVIER FOR STA CRUZ CASEAndee SalegonNo ratings yet
- FNCP (Hypertension)Document3 pagesFNCP (Hypertension)Jose Emmanuel Ribaya RuivivarNo ratings yet
- Gensurvey SJMCDocument2 pagesGensurvey SJMCMariKeith AcostaNo ratings yet
- Cardiovascular Conditioning Monitoring ChartDocument2 pagesCardiovascular Conditioning Monitoring ChartDanielle Patricia Valencia OtedaNo ratings yet
- NCP Acute Pain FURUNCOLOSISDocument2 pagesNCP Acute Pain FURUNCOLOSISMaria Imogen MilambilingNo ratings yet
- FNCPDocument5 pagesFNCPCarina QuibinitNo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitPrincess Faniega SugatonNo ratings yet
- Saldana - Fdar Lung CancerDocument2 pagesSaldana - Fdar Lung CancerMika SaldañaNo ratings yet
- Case IcuDocument5 pagesCase IcuTrisha SuazoNo ratings yet
- Nursing Care Plan: Cues Problem Scientific Reason Nursing Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Cues Problem Scientific Reason Nursing Intervention Rationale Evaluationeihjay-bravo-8041No ratings yet
- SJMC - xi-nCP&HTP - Impaired Skin IntegrityDocument10 pagesSJMC - xi-nCP&HTP - Impaired Skin IntegrityJoy CompetenteNo ratings yet
- Impaired Skin IntegrityDocument3 pagesImpaired Skin IntegrityAubrey SungaNo ratings yet
- SDL3Document2 pagesSDL3Margaux BaynosaNo ratings yet
- NCP DM Group 6Document4 pagesNCP DM Group 6Jeffrey Calicdan BucalaNo ratings yet
- NCP Readiness RevisionDocument3 pagesNCP Readiness RevisionimnasNo ratings yet
- Impaired Tissue Integrity BurnDocument1 pageImpaired Tissue Integrity BurntabaloveNo ratings yet
- Nursing Care Plan: References: Nurse's Pocket Guide Pages 151-155Document1 pageNursing Care Plan: References: Nurse's Pocket Guide Pages 151-155Caroline ChaNo ratings yet
- NCP (Acute Pain)Document2 pagesNCP (Acute Pain)jennilois100% (1)
- Llacer FdarDocument2 pagesLlacer FdarRaidis PangilinanNo ratings yet
- Actual NCPDocument3 pagesActual NCPcarmaxeta100% (2)
- NCP Acabo Hypokalemia 1Document2 pagesNCP Acabo Hypokalemia 1Doneva Lyn MedinaNo ratings yet
- FDAR (After Tracheostomy)Document2 pagesFDAR (After Tracheostomy)Maribeth DantesNo ratings yet
- Common Nursing Diagnosis Found in Nursing Care Plans For HypertensionDocument2 pagesCommon Nursing Diagnosis Found in Nursing Care Plans For HypertensionRaveen mayiNo ratings yet
- NCP Icu-CcuDocument6 pagesNCP Icu-CcuJohn CenasNo ratings yet
- Nursing Care Process (NCP) Stress Overload PrepartumDocument2 pagesNursing Care Process (NCP) Stress Overload PrepartumFrederene JavelonaNo ratings yet
- FNCP TB As A Health DeficitDocument5 pagesFNCP TB As A Health Deficitkuu faalNo ratings yet
- Acute Pain OsteosarcomaDocument8 pagesAcute Pain OsteosarcomaMaryjoy Gabriellee De La Cruz100% (1)
- "Hindi Ko Kayo Masyadong Marinig Sa Kanang Tenga Ko, Pwede Bang Sa Kaliwang Side Ko Kayo Magsalita?" As Verbalized by The PatientDocument2 pages"Hindi Ko Kayo Masyadong Marinig Sa Kanang Tenga Ko, Pwede Bang Sa Kaliwang Side Ko Kayo Magsalita?" As Verbalized by The PatientMussaib Mushtaq100% (1)
- Discharge Plan CapDocument3 pagesDischarge Plan Capalexander abasNo ratings yet
- RISK For INJURY Related To Regulatory Function (Sensory Difunction As Evidenced by Decrease Visual Acuity, Unable To Recognize Object 12-14 Inches Away, Not Wearing of Eyeglasses.Document2 pagesRISK For INJURY Related To Regulatory Function (Sensory Difunction As Evidenced by Decrease Visual Acuity, Unable To Recognize Object 12-14 Inches Away, Not Wearing of Eyeglasses.Senyorita KHayeNo ratings yet
- NCP Acute Pain FractureDocument1 pageNCP Acute Pain FractureAi RouNo ratings yet
- Anemia NCP and HTPDocument8 pagesAnemia NCP and HTPChad Smith100% (1)
- NCP DobDocument2 pagesNCP DobPaulo GeneraloNo ratings yet
- Drug Study: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument2 pagesDrug Study: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesNikki Caryl ZafraNo ratings yet
- NCP For Risk For Acute PainDocument3 pagesNCP For Risk For Acute PainAngelgodess Athena-envyNo ratings yet
- Final Course in The WardDocument4 pagesFinal Course in The WardMichael Boado100% (1)
- Opstres Maalox Benutrex-C Paracetamol Essentiale Forte BactidolDocument6 pagesOpstres Maalox Benutrex-C Paracetamol Essentiale Forte Bactidolpark nisseNo ratings yet
- NCPDocument3 pagesNCPMichael John F. NatividadNo ratings yet
- Ncp'sDocument8 pagesNcp'sDuchess Kleine RafananNo ratings yet
- Head Nurse: General ObjectiveDocument10 pagesHead Nurse: General Objectiveeihjay-bravo-8041No ratings yet
- HTP PneumoniaDocument2 pagesHTP PneumoniaNikki ArmentaNo ratings yet
- ASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoDocument1 pageASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoCherie MayNo ratings yet
- Icu NCPDocument4 pagesIcu NCPdrsabuegNo ratings yet
- NPI Mariano Psychiatric WardDocument4 pagesNPI Mariano Psychiatric WardAlessandra Dominique MarianoNo ratings yet
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- Nursing Care Plan For Breast Cancer NCP PDFDocument2 pagesNursing Care Plan For Breast Cancer NCP PDFMaina BarmanNo ratings yet
- NCP Impaired Physical MobilityDocument1 pageNCP Impaired Physical MobilityCharmaine SolimanNo ratings yet
- Surgery JournalDocument1 pageSurgery JournalPhilippe CANTORIA (SHS)No ratings yet
- NCP TahbsoDocument18 pagesNCP TahbsoKe EjieNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument2 pagesNursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDat boiNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument2 pagesNursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveGaurav Gaikwad100% (3)
- Actual Nursing Care PlanDocument2 pagesActual Nursing Care Planshaileene bugayongNo ratings yet
- NCPDocument2 pagesNCPjoyce_albertoNo ratings yet
- RI Family Support Specialists: Navigating The Way To Resources, Support and Better Outcomes For Children and Families (Joanne Quinn)Document1 pageRI Family Support Specialists: Navigating The Way To Resources, Support and Better Outcomes For Children and Families (Joanne Quinn)AUCDNo ratings yet
- Chapter 2 Solution 1Document4 pagesChapter 2 Solution 1Pragya PandeyNo ratings yet
- Indifference CurveDocument32 pagesIndifference CurveSalvia AhmadNo ratings yet
- March 16 - Mohit - CBE 741Document59 pagesMarch 16 - Mohit - CBE 741Mohit bibraNo ratings yet
- Rainfll Measure VoterDocument15 pagesRainfll Measure VoterngaNo ratings yet
- Test Bank For Introduction To Communication Disorders 5th Edition by OwensDocument34 pagesTest Bank For Introduction To Communication Disorders 5th Edition by Owensmammalconsols7z84100% (47)
- Hikam Commentary IntroDocument1 pageHikam Commentary IntroNik RoskimanNo ratings yet
- Bookshoppe Jan 2013Document23 pagesBookshoppe Jan 2013ibnusina2013No ratings yet
- John Walvoord InterpretationDocument26 pagesJohn Walvoord InterpretationsekarjoshuaNo ratings yet
- Exam 2Document6 pagesExam 2María Belkis Rozo MeloNo ratings yet
- Marathi Verb Morphology and POS Tagger: Veena DixitDocument10 pagesMarathi Verb Morphology and POS Tagger: Veena DixitarjunNo ratings yet
- M1 MarkschemeDocument17 pagesM1 MarkschemeShere AhmedNo ratings yet
- OBLICON - Sta Maria Reviewer 2010-2011Document92 pagesOBLICON - Sta Maria Reviewer 2010-2011anna_bueno91% (11)
- Family LW Iringa University CollegeDocument51 pagesFamily LW Iringa University CollegeRANDAN SADIQNo ratings yet
- The Charters ModelDocument10 pagesThe Charters ModelKamaladharanii Ragu Nathan50% (2)
- TRUST AND OBEY Victory in Jesus Marvelous Grace City of Gold Paid in FullDocument94 pagesTRUST AND OBEY Victory in Jesus Marvelous Grace City of Gold Paid in FullVincent MadrideNo ratings yet
- Mapping Toolbox GuideDocument1,710 pagesMapping Toolbox GuideAaron RampersadNo ratings yet
- Psalm 24: Unity in Diversity I P J Botha (UP)Document11 pagesPsalm 24: Unity in Diversity I P J Botha (UP)Johnny HannaNo ratings yet
- First Voyage Around The World by Magellan W2P1Document32 pagesFirst Voyage Around The World by Magellan W2P1Maria Reynagie Ogue0% (1)
- Social Media and Its Influence On Public OpinionDocument8 pagesSocial Media and Its Influence On Public Opiniongirish karuvelilNo ratings yet
- Dme-II Question BankDocument4 pagesDme-II Question BankenggsantuNo ratings yet
- Descargar Imagenes Iso de Juegos Ps2Document18 pagesDescargar Imagenes Iso de Juegos Ps2Gandhy LeónNo ratings yet
- Memorial On Behalf of The AppellantDocument30 pagesMemorial On Behalf of The Appellantbhumikabisht3175No ratings yet
- Contemplative PrayerDocument10 pagesContemplative PrayerPhoyCfc SpcNo ratings yet
- Chapter 04Document19 pagesChapter 04erza scarletNo ratings yet